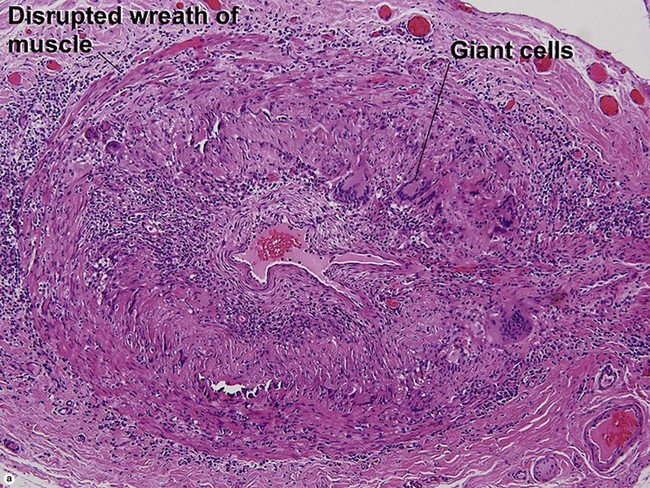
Chapter 11 Granulomatous arteritis involving the aorta and its major branches. Usually <50 years of age.
Inflammatory vascular diseases
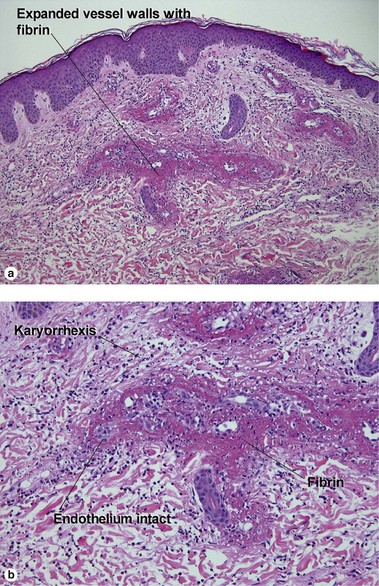
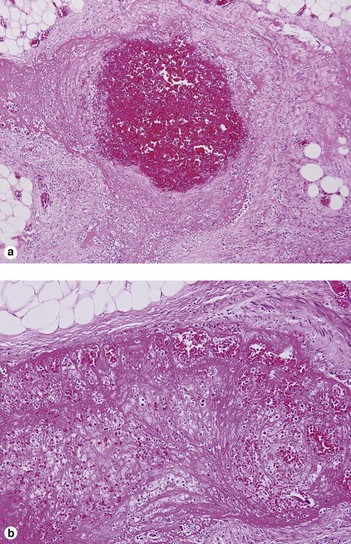
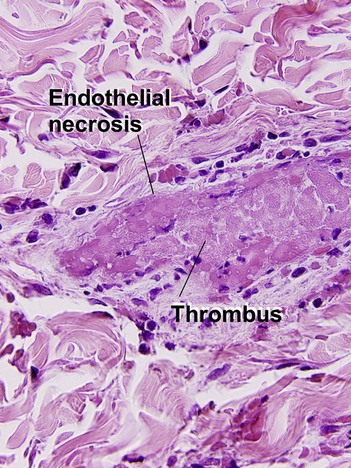
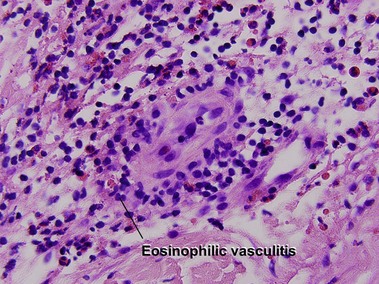
Leukocytoclastic vasculitis (LCV)
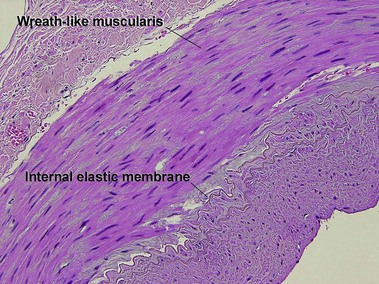
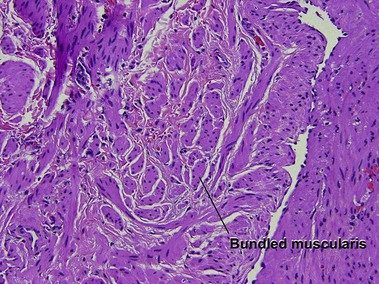
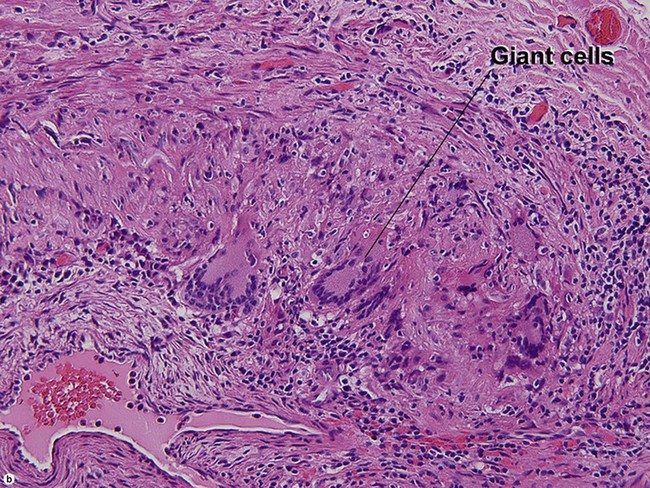
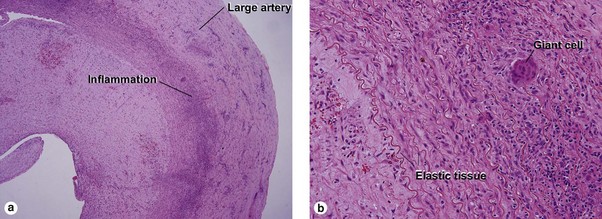
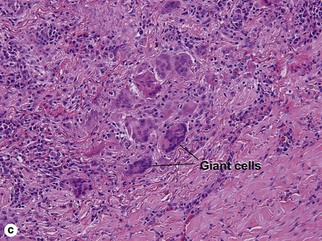
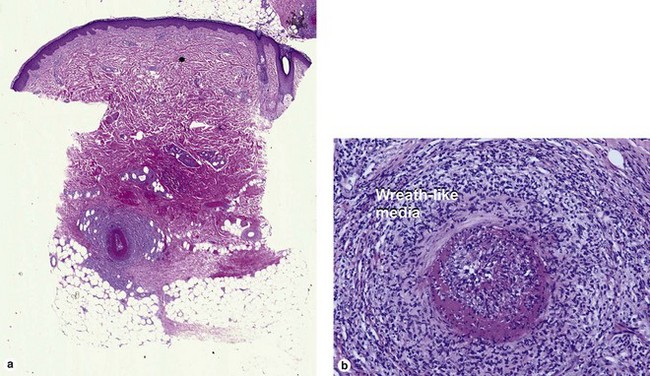
Large vessel vasculitis
Takayasu arteritis
Chapel Hill criteria
Inflammatory vascular diseases