, Teresa S. Wright2, Crystal Y. Pourciau3 and Bruce R. Smoller4
(1)
Department of Pathology & Immunology, Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas, USA
(2)
Departments of Dermatology and Pediatrics, University of Tennessee Health Science Center, Memphis, TN, USA
(3)
Departments of Dermatology and Pediatrics, Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas, USA
(4)
Department of Pathology and Laboratory Medicine, University of Rochester School of Medicine and Dentistry, Rochester, NY, USA
10.1 Miliaria
10.1.1 Clinical Features
Miliaria (prickly heat ) is the cutaneous manifestation of occlusion of eccrine sweat glands and may occur in up to 15 % of newborns [1]. Predisposing factors include warm, humid environments, fever and excessive bundling.
Lesions tend to occur in areas of the body that are occluded, such as the torso, but may occur on the forehead and cheeks as well. The palms or soles are rarely affected [1]. Patients present with monomorphic, erythematous papules, pustules or vesicles, some of which may have associated induration with morphology dependent upon the level of obstruction within the eccrine unit (Fig. 10.1). Miliaria typically resolves within hours to days following removal of the exacerbating condition. No residual dyschromia or other cutaneous sequelae are expected.

Fig. 10.1
Miliaria crystallina is characterized by non-follicular-based skin-colored papules and vesicles on the upper torso of a child
10.1.2 Histology
Miliaria represents a spectrum of eruptions that are characterized by disruption of the eccrine ducts at various points throughout the outflow tract with extravasation of secretions. Histologically, the site of disruption results in slightly different histologic patterns.
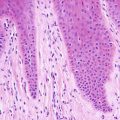
Miliaria crystallina is a form of the condition in which the disruption in the sweat duct is closest to the surface of the skin. In this condition, secretion is present at the level of the acrosyringia within the stratum corneum, resulting in intracorneal fluid collections and focal epidermal spongiosis . Inflammation is usually minimal, and it is believed to be a secondary part of the process (Fig. 10.2). Neutrophils are the predominant type of inflammatory cells present (Fig. 10.3) [2, 3].
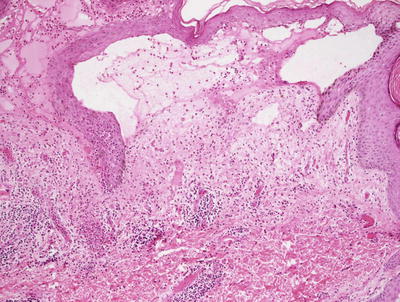
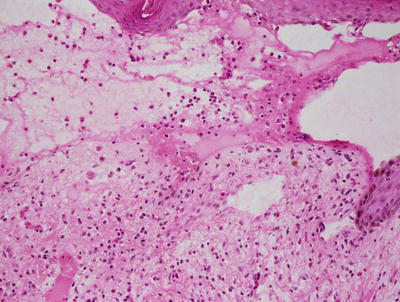
Fig. 10.2
Areas of papillary dermal edema and a mixed inflammatory infiltrate are seen in miliaria crystallina
Fig. 10.3
Neutrophils and eosinophils accompany lymphocytes in the inflammatory infiltrate seen in miliaria crystallina
Miliaria rubra is a variant in which the leakage of secretion occurs in the intraepidermal portion of the eccrine ducts. Secretion is present within the epidermis resulting in marked spongiosis. Inflammation is usually not striking (Fig. 10.4) [4].
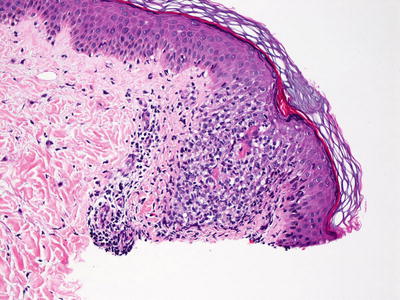
Fig. 10.4
Miliaria rubra demonstrates spongiosis within the epidermis surrounding an acrosyringium
Miliaria profunda is the most deep-seated variant of the entity with leakage of secretion occurring within the dermis. A lymphocytic inflammatory infiltrate may be present in some cases. In rare cases, large areas with miliaria profunda may present as dermal plaques and histologic findings demonstrate a granulomatous reaction to the extravasated eccrine secretions [5, 6].
10.1.3 Pathogenesis
Miliaria is caused by occlusion of the sweat duct with extravasation of sweat into the surrounding tissue as well as increased bacterial colonization and subsequent inflammatory reaction [4, 7–9]. Clinical variants include miliaria crystallina, miliaria rubra, and miliaria profunda, and the variant depends on the anatomic location of obstruction in the eccrine duct.
10.2 Erythema Toxicum Neonatorum
10.2.1 Clinical Features
Erythema toxicum neonatorum is common, reportedly occurring in 50–70 % of full-term infants [1]. It appears to have a much lower incidence in preterm and low birth weight newborns. Only 5 % of cases are congenital with most lesions occurring within the first 24–48 hours of life.
Physical exam is characterized by erythematous wheals, papules, pustules, and macules with predilection for the face, torso, proximal extremities, and buttocks. Lesions rarely occur on the palms or soles. The eruption may wax and wane with individual lesions lasting anywhere from a few hours to days. The disease is a self-limited process and typically resolves within 1 week of life with no residual changes in the skin [1].
10.2.2 Histology
Erythema toxicum neonatorum is characterized by subcorneal or intraepidermal pustules of eosinophils and marked inflammation within the pilosebaceous unit, usually at a level just deep to the dermal-epidermal junction [10, 11]. The inflammatory response may also be present in the surrounding dermis. A scant perivascular inflammatory infiltrate with scattered eosinophils is present in the dermis in some cases. Some authors have suggested that erythema toxicum neonatorum may be closely related to transient neonatal pustular melanosis [12, 13].
10.2.3 Pathogenesis
Erythema toxicum neonatorum may represent a type of cutaneous immunological response to microbial colonization of the hair follicles in the first few days of life of the newborn. A number of proinflammatory molecules have been identified, including interleukin-1 (IL-1), IL-8, eotaxin, aquaporin, psoriasin, and nitric oxide synthase [14]. Other etiologies have been proposed, including the presence of enterotoxins in the newborn, allergic response to transplacental allergens, and response to external stimuli [14, 15].
10.3 Milium
10.3.1 Clinical Features
Milia can be subcategorized into primary and secondary variants with the latter occurring in response to trauma, while the former is idiopathic [16]. Milia are frequently seen in infancy, occurring in 40–50 % of term neonates with delayed onset or lower incidence in premature infants [16]. Primary milia also are seen in children and adults, although lesion distribution on clinical exam varies from that of infantile onset. No racial or gender predilection exists in any studied age group.
Classically, milia are described as 1–2 mm, smooth surfaced white papules. In infants, milia present on the central face, scalp, upper trunk, and upper extremities [16]. In children and adults, milia are more commonly found on the eyelids, cheeks, forehead, and genitalia. Atypical variants exist, including milia en plaque, multiple eruptive milia, and nodular grouped milia. Milia are self-resolving and usually abate within several weeks to months. Treatment is typically not required, but cyst evacuation can be performed easily.
10.3.2 Histology
It is generally believed that primary milia arise from the pilosebaceous units and secondary milia arise from the eccrine ducts [16, 17]. The histologic features can be used to delineate the nature of the milia. Primary milia resemble very small infundibular follicular cysts. Small cystic dilatations are lined by epidermis containing a granular layer and are filled with keratin. These tend to occur in the region of the insertion of the sebaceous ducts into the pilosebaceous units [16]. Secondary milia are also cystically dilated spaces, but the cystic cavities are lined by ductal epithelium. Serial sectioning demonstrates connections to eccrine ducts in most cases [18].
10.4 Acne Neonatorum
10.4.1 Clinical Features
Acne neonatorum is thought to occur in ~20 % of healthy infants. Lesions may be present at birth, but they usually occur within the first 2 weeks to 2 months of life [1]. Male infants appear to be more commonly affected than female infants [19]. Neonatal cephalic pustulosis is thought to be a subset of acne neonatorum seen in the first few months of life. It is likely to be an inflammatory response to skin colonization by pityrosporum yeast (Malassezia species) [1].
In acne neonatorum and neonatal cephalic pustulosis, the primary lesion is an erythematous papule or pustule with multiple lesions scattered on the face, scalp, and neck (Fig. 10.5). In acne neonatorum, while papules and pustules may be seen, comedones (open and closed) and cystic nodules are present as well. Lesions are typically localized to the face. Acne neonatorum and neonatal cephalic pustulosis usually resolve spontaneously within months, and they do not require medical therapy. However, acne neonatorum can be more persistent and inflammatory, predisposing patients to scarring. Hence, a subset of these patients may benefit from treatment.

Fig. 10.5
Erythematous papules and skin-colored comedones on the central face of a child with acne neonatorum (photo courtesy of Minh Hoang, MD, Ho Chi Minh City, Vietnam)
10.4.2 Histology
Histologic findings in acne neonatorum are indistinguishable from acne vulgaris , and the entity is defined solely upon the clinical presentation. Changes include dilatation of follicular ostia, keratin plugs, and variable amounts of perifollicular lymphohistiocytic inflammation. Sebaceous hyperplasia has been described. In more florid cases with rupture of the pilosebaceous units, the perifollicular infiltrate may be granulomatous [20].
10.4.3 Pathogenesis
Acne neonatorum often occurs during the first few weeks of life. Sebaceous hyperplasia is present in the lesions, and this is thought to be secondary to the effects of maternal hormones and infant androgens on the neonate’s sebaceous glands [21]. There is a strong male predominance in acne neonatorum. Neonatal adrenal glands are hyperactive, producing β-hydroxysteroids and particularly in male infants, there is also production of luteinizing hormone and testosterone [20, 22–24]. Sebaceous glands in acne neonatorum are hypertrophic with increased hydroxysteroid dehydrogenase activity and sebum production, similar to sebaceous changes in puberty [20]. Pityrosporum ovale has been identified in neonatal cephalic pustulosis, suggesting a possible infectious factor in the pathogenesis of acne neonatorum [25].
10.5 Acne Vulgaris
10.5.1 Clinical Features
Acne affects 85 % of young adults between 12 and 24 years old [26]. People of all ethnicities and racial backgrounds are affected. Symptoms correlate best with pubertal age. The disease is seen infrequently in children from 1 to 7 years old and less commonly in older adults.
The comedo is the primary lesion of acne vulgaris, but affected individuals can have a mixed eruption of comedones with erythematous papules , pustules, and cystic nodules, primarily occurring on the face, chest, and back. Dyschromia and scarring are sequelae seen in response to more inflammatory disease. Severity of acne vulgaris is graded and determined by the type and number of lesions present as well as the distribution of lesions (Fig. 10.6).

Fig. 10.6
Multiple erythematous papules, pustules, and cystic nodules admixed with atrophic scars are seen in a teenage boy with acne conglobata
Acne conglobata represents a severe suppurative variant of acne vulgaris. It is seen more often in males between 18 and 30 years of age and in those of African descent [26]. Patients with acne conglobata universally present with painful cystic nodules on the face, chest, and back that heal with hypertrophic scarring. In acne fulminans, patients have acne as well as systemic complaints of fever, malaise, and arthralgia. Acne conglobata and acne fulminans are often refractory to treatment and have greater associated morbidity. These variants can be a feature of other systemic inflammatory conditions, such as SAPHO syndrome (Synovitis, Arthritis, Acne, Pustulosis, Hyperostosis, Osteitis).
10.5.2 Histology
The changes of acne vulgaris include sebaceous hyperplasia and varying degrees of inflammation within and around the pilosebaceous units. Mild cases may demonstrate only a scant lymphohistiocytic infiltrate at the level of the follicular infundibulum with focal follicular spongiosis. More florid cases will show comedones with cystic dilatation of the follicular ostia with keratin plugging (Figs. 10.7 and 10.8). Neutrophilic abscesses can be found within follicular outflow tracts or in the adjacent dermis. Follicular plugging can result in the development of follicular cysts, and in some cases accompanied by marked inflammation. In more extensive cases, there may be disruption of the follicular epithelia, extrusion of keratin into the dermis, and marked inflammation. A granulomatous response with multinucleated giant cells and abundant histiocytes is not unusual in these cases.
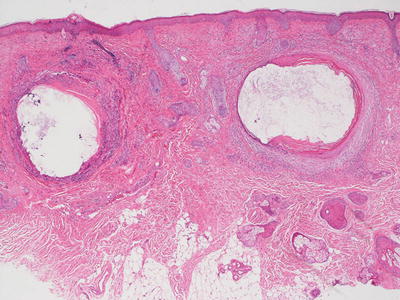
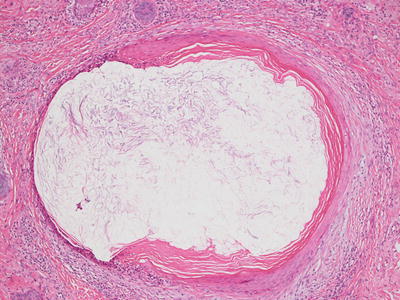
Fig. 10.7
Dilated keratin-filled follicles are surrounded by an inflammatory infiltrate in acne vulgaris
Fig. 10.8
Keratin fills a cystically dilated hair follicle in a comedone in acne vulgaris
The histologic findings in acne conglobata are shared with those seen in other conditions including hidradenitis suppurativa. There is marked follicular plugging resulting in multiple follicular cysts that can be quite large (Fig. 10.9). These cysts are surrounded by dense inflammation including lymphocytes, neutrophils, and often granulomas with abundant multinucleated giant cells. As a result of repeated rupture of follicular cysts, there is extensive dermal scarring and even sinus tract formation (Fig. 10.10).
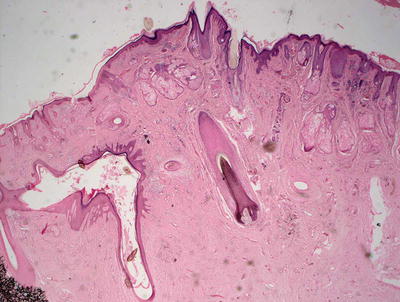
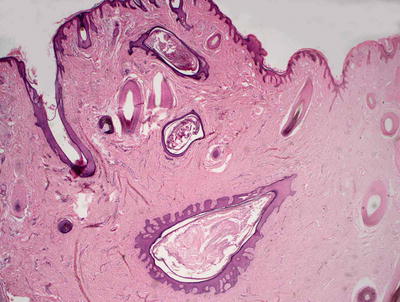
Fig. 10.9
Acne conglobata shows marked distortion of pilosebaceous units with dense scar formation
Fig. 10.10
Abundant pilosebaceous units are disrupted and surrounded by dense scarring throughout the dermis in acne conglobata
10.5.3 Pathogenesis
Comedone formation can be induced by Propionibacterium acnes overgrowth, hormones (androgens), and lipid composition in sebocytes as well as local cytokines [28, 29]. P. acnes are gram-positive anaerobic bacteria that reside in the hair follicles in the skin with resultant sebum accumulation and follicular rupture due to bacterial proliferation and associated local inflammatory reaction [28, 30]. The inflammatory response is a major mechanism behind acne vulgaris. Interleukin-1α (IL-1α) is an important cytokine for comedone formation by increasing sebum production and decreasing linoleic acid (which is important in skin barrier function) [31, 32]. P. acnes can induce IL-1α production [28, 33]. Blockade of IL-1α receptor results in the inhibition of follicular hyperkeratinization . Hyperkeratinization and plugging of the follicular infundibulum form comedones, which are the initial lesions of acne vulgaris.
The composition of sebum lipids produced by sebaceous glands can influence inflammation in acne vulgaris. Sebum typically consists of lipids and cholesterols (triglycerides, free fatty acids, wax esters, squalenes, cholesterol, and cholesterol esters) [34]. Changes in the composition of sebum have been associated with follicular hypercornification and acne formation [35, 36]. Lipid peroxidation products can promote inflammatory cytokines (such as IL-1α) and recruitment of inflammatory cells [37]. Sebum lipids also promote the growth of P. acnes , and lipases produced by P. acnes hydrolyze triglycerides into pro-inflammatory free fatty acids [38]. Recent studies have indicated that peroxisome proliferator-activated receptor-γ (PPAR-γ) may serve a protective role in acne vulgaris by preventing excessive accumulation of lipids in sebaceous glands [39].
Acne conglobata is a highly inflammatory form of acne . It is a chronic inflammatory disease with occlusion of the hair follicles [40]. Propionibacterium acnes stimulates keratinocytes to produce IL-1α and tumor necrosis factor (TNF)-α [41, 42]. These pro-inflammatory cytokines are important in the pathogenesis of acne conglobata. TNF-α antagonists have been used in the treatment of acne conglobata [42]. Other studies have revealed additional important factors, such as the modulation of toll-like receptor-4 (TLR4) as a new therapeutic option for severe forms of acne conglobata [43].
10.6 Drug-Induced Acne
10.6.1 Clinical Features
Drug-induced acne (acne medicamentosa) is thought to occur following exposure to systemic glucocorticoids, but it has been associated with a number of other medications, including halogenated compounds, antiepileptic drugs (phenytoin, carbamazepine, and gabapentin), antidepressants (lithium), antitubercular drugs (isoniazid), growth hormone, cyclosporine, contraceptives (medroxyprogesterone), and anabolic steroids (danazol, and testosterone) [44]. A number of chemotherapies have been associated with acneiform eruptions as well, most notably epidermal growth factor-receptor (EGFR) inhibitors and other inhibitors of oncogenic pathways (RAS/RAF/MEK/ERK) [44]. The acneiform eruptions in these cases appear to be dose-dependent and occur almost universally in patients receiving the medication.
Acneiform eruptions secondary to drug exposure frequently are monomorphic with follicular-based papules and papulopustules at the trunk and proximal arms, and comedones are infrequently seen, thus distinguishing this variant of drug eruption from acne vulgaris (Fig. 10.11). In chemotherapy-associated acne, lesions tend to occur within the first 2 to 4 weeks of therapy [44]. Pruritus is a frequent complaint, and more lesions are seen on the head and neck in addition to the upper trunk. These lesions frequently resolve once the inciting agent is removed.

Fig. 10.11
Steroid-induced acne is characterized by monomorphic, erythematous, follicular-based papules primarily localized to the trunk
10.6.2 Histology
The histologic changes in drug-induced acne cannot be readily distinguished from those occurring in acne vulgaris. Some authors describe a predominance of a neutrophilic infiltrate in steroid-induced acne [45], but neutrophils are also prominent in many cases of acne vulgaris. Clinical presentation is the best way to make this distinction.
10.6.3 Pathogenesis
A number of drugs can induce acne formation. However, the mechanism of drug-induced acne is not known. Steroids , such as glucocorticoids , can induce toll-like receptor-2 (TLR-2) expression in human keratinocytes . Propionibacterium acnes and hormones , such as androgenic or anabolic steroids and estrogen, can induce acne [46–48]. Immunosuppressants , anticonvulsant medications and psychotropic drugs can also cause acne [47].
10.7 Acne Rosacea
10.7.1 Clinical Features
Rosacea sometimes occurs in children, but it more commonly affects men and women over 30 years old [44]. Rosacea is distinguished from acne vulgaris based upon the absence of comedones. Patients typically present with erythematous papules, pustules, and cystic nodules on the central face (Fig. 10.12). Additional presentations in childhood rosacea include facial flushing and persistent telangiectasias, as well as ophthalmologic symptoms, such as blepharitis, meibomianitis, recurrent chalazion (most commonly seen), episcleritis, iritis, and corneal ulceration, neovascularization and scarring [44, 49]. While it appears that cutaneous disease responds well to medical therapy, associated ophthalmologic symptoms may predispose affected children to irreversible vision impairment if the condition is not recognized and managed appropriately [49].

Fig. 10.12
Acne rosacea in a young adolescent girl with erythematous papules and pustules on the central face
10.7.2 Histology
Acne rosacea demonstrates a perifollicular lymphohistiocytic infiltrate with spongiosis at the level of the infundibulum (Fig. 10.13). Sebaceous hyperplasia is present in many cases. Florid cases may have a granulomatous inflammatory response to ruptured follicular epithelium (Figs. 10.14 and 10.15).
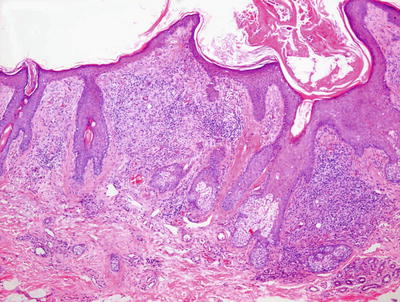
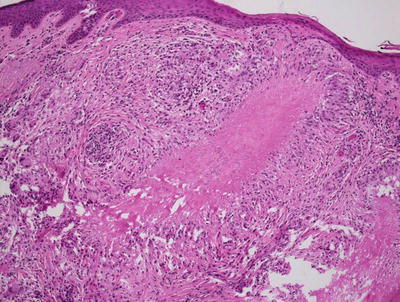
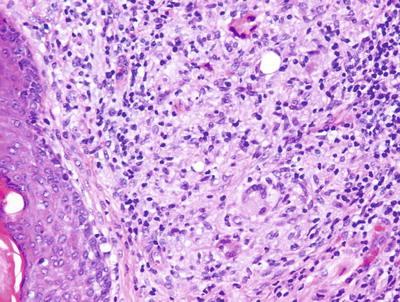
Fig. 10.13
Granulomas with multinucleated giant cells located in the region of pilosebaceous units are characteristic of acne rosacea
Fig. 10.14
A caseating granuloma is present in acne rosacea
Fig. 10.15
Granulomas adjacent to follicular units are a diagnostic feature of acne rosacea
The major histologic differential diagnosis is lupus erythematosus. The presence of an interface dermatitis, epidermal atrophy, diffuse hyperkeratosis, basement membrane thickening, and dermal mucin may all be seen in lupus erythematosus, and these are not characteristic findings in acne rosacea. A peri-eccrine infiltrate would also favor a diagnosis of lupus erythematosus. However, as these findings are not all present in every case, histologic distinction may be difficult.
Acne vulgaris might also enter the differential diagnosis, and there is great overlap in histologic changes. The presence of marked follicular plugging is more common in acne vulgaris. However, in most cases, clinical presentation is the best way to make this distinction.
10.7.3 Pathogenesis
Rosacea is a chronic inflammatory condition of the facial skin. The pathogenesis of rosacea involves kallikrein 5, a trypsin-like serine protease, which is thought to initiate an augmented inflammatory response in rosacea [50]. Increase in kallikrein 5 results in increased production of the cathelicidin peptide LL-37 , which is an antimicrobial peptide that provides innate defense immunity against several microbial organisms. LL-37 stimulates inflammation, vasodilation, and angiogenesis, which are characteristic features of the disorder [50]. Patients with rosacea have high levels of LL-37 in the facial skin, with corresponding increase in kallikrein 5 that cleaves an inactive precursor protein into LL-37, which is a pro-inflammatory and pro-angiogenic peptide [51–54]. Injection of LL-37 peptide fragments into animal skin elicits an inflammatory response similar to rosacea [53]. Agents that inhibit kallikrein 5 and the production of LL-37 peptides, such as azelaic acid and doxycycline, are effective in reducing cutaneous lesions in rosacea [55, 56].
Toll-like receptors (TLRs) are tightly bound to innate immunity. The expression of TLR2 is increased in rosacea [57]. Through TLR2, the production of serine proteases, such as kallikrein 5, is increased with subsequent increase in LL-37 levels [58, 59]. Ultraviolet (UV) light radiation is a well-known trigger of rosacea. UV light induces the formation of reactive oxygen species (ROS) in skin [60]. The interaction of ROS with TLR2 leads to increased levels of pro-inflammatory chemokines and cytokines that contribute to the pathogenesis of rosacea.
The inflammatory cytokine and chemokine network in rosacea has been under investigation. External and internal trigger factors that induce pro-inflammatory cytokines , such as tumor necrosis factor-α (TNF-α) and interleukin-1 (IL-1) , leads to the recruitment of type 1 T-help cells (Th1) and IL-17-producing T-helper cells (Th17) to facial skin [61]. T lymphocyte-derived cytokines IL-17 and IL-22 can facilitate neutrophil recruitment to the skin. IL-17 promotes angiogenesis by inducing vascular endothelial growth factor (VEGF) and other pro-angiogenic factors. LL-37 can induce the chemokine CXCL8, which is a potent chemo-attractant of neutrophils, leading to the formation of sterile pustules in a mouse model of rosacea [62].
In rosacea, there is dysregulation of the neurovascular/neuroimmune system and the immune response. The neurovascular/neuroimmune system contributes to the pathogenesis of rosacea by enhancing vasodilation of the skin vasculature as well as the associated neurosensory symptoms [63–66]. VEGF may mediate the vascular changes and vascular proliferation that occur in rosacea [59, 67]. Vasoactive intestinal peptide (VIP) receptor (which is increased in skin blood vessels in phymatous rosacea) and substance P (which is a neuropeptide involved in local blood flow regulation) have also been linked to rosacea [68, 69]. Rosacea skin also has lower heat pain threshold than normal skin [59]. Various subtypes of transient receptor potential ion channels of the vanilloid type (TRPV) , which are cellular sensors of cold, heat, and pain sensation, may be involved in rosacea. Interestingly, the expression of TRPVs is significantly increased in rosacea [70].
10.8 Fox-Fordyce Disease
10.8.1 Clinical Features
Fox-Fordyce disease (also known as apocrine miliaria) is a chronic pruritic papular eruption of the apocrine gland-bearing areas of the body [71]. It more commonly occurs in post-pubescent females with an age range of 13–35 years of age [71, 72].
On physical exam, patients have pruritic, dome-shaped, skin-colored to erythematous papules primarily at the axillae, mammary areolae, pubis, and gluteal fold [71]. Papules are follicular-based, although non-follicular-based papules secondary to occlusion of apo-eccrine ducts have been reported [71]. The disease may be difficult to manage and may require surgical intervention in patients with more severe presentation and who are refractory to standard topical medications [73].
10.8.2 Histology
Histologic features seen in Fox-Fordyce disease include intraepidermal fluid-filled vesicles within the outflow tracts of apocrine ducts, as well as hyperkeratosis and spongiosis at the infundibular level of the hair follicle, and foamy macrophages [74, 75]. The foamy macrophages are seen in the region immediately surrounding the pilosebaceous unit and may be associated with prior rupture and extravasation of ductal secretions. Hyperkeratosis, follicular dilatation with keratin plugging, focal dyskeratosis, and basal vacuolization along the follicular epithelium have also been described in some cases [74, 76]. In longer standing lesions, perifollicular fibrosis and a surrounding lymphohistiocytic infiltrate are prominent [77].
10.8.3 Pathogenesis
Fox-Fordyce disease in a chronic inflammatory disorder of the skin involving apocrine glands and keratin plugging of the follicular infundibulum at the distal portion of the apocrine sweat duct [71]. Hormonal factors appear to play a role since the disease occurs more commonly in females with 90 % of the cases occurring in individuals between 13 and 35 years of age [78]. Fox-Fordyce disease occurs with the onset of puberty, flares up during menstrual periods, and improves during pregnancy, after menopause, and with use of oral contraceptives [79]. There are reports of Fox-Fordyce disease in prepubertal girls, suggesting that the cause is probably multifactorial and not solely hormone-based [72]. Obstruction of apocrine ducts with keratin plugs can result in sweat retention and subsequent rupture of the obstructed duct, leading to inflammation [80]. Botulinum toxin type A , which inhibits sweat secretion by causing chemical denervation of cholinergic nerve terminals to eccrine and apocrine glands, has been used successfully to treat refractory disease [81].
10.9 Hidradenitis Suppurativa
10.9.1 Clinical Features
Hidradenitis suppurativa is a chronic condition of the intertriginous skin, now thought to be an obstructive inflammatory process of the hair follicle with subsequent involvement of the adjacent apocrine glands [82]. Hidradenitis suppurativa is seen almost universally in postpubertal individuals with average age of onset between 20 and 30 years of age [83]. Prevalence rates vary with range up to 4 %, depending upon the population studied [83]. The disease appears to occur more commonly in females. No substantiated racial predilection has been demonstrated consistently. Both smoking and obesity have strong associations with disease occurrence and exacerbation.
Physical exam is notable for double comedones, subcutaneous nodules, and fluctuant cysts at the axillae anogenital regions (inguinal, pubis, perianal, and perineal) and the chest (intra- and infra-mammary breasts) with potential for evolution to sinus tract formation and fibrosis. The axillae are the most commonly affected site, while perianal disease has the greatest associated morbidity [83]. Skin lesions have been reported at the occiput and posterior neck as well [84]. Disease may be graded using the Hurley Staging System (I–III) , which is based on number of lesions seen, the presence of tract formation and scarring, and the distribution of affected area.
Hidradenitis suppurativa can be difficult to manage with therapy plans dependent on the chronicity and severity of disease. Notable reported sequelae and disease complications include impaired quality of life (with associated economic, psychosocial, and physical disability), contractures, mucosal strictures, and lymphedema at sites of prolonged inflammation and scarring [83]. Additionally, increased incidence of squamous cell carcinoma and other skin malignancies have been reported in more severely affected individuals.
10.9.2 Histology
Hidradenitis suppurativa in its earliest phase demonstrates an infundibulofolliculitis [85, 86]. Spongiosis and a lymphocytic infiltrate occur secondary to keratin plugs occluding the outflow tracts of hair follicles. It is generally believed that the occlusion of apocrine ducts, and cystic dilation and rupture are secondary events, and occur later in the development of the disease process. The marked inflammation that ensues is secondary, and it is often granulomatous in nature and inevitably leads to scar formation as well as the development of sinus tracts in well-established lesions (Fig. 10.16). Diminished numbers of sebaceous glands have been described in biopsies from patients with hidradenitis suppurativa, but this finding may be secondary to the chronic inflammation and scar formation characteristically extend deep into the subcutaneous fat [87, 88].
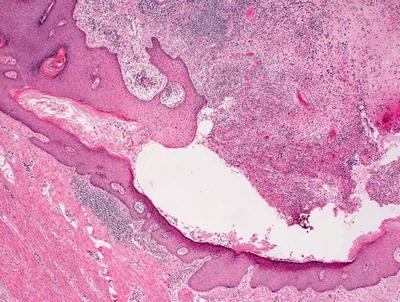
Fig. 10.16
Ruptured pilosebaceous units with abscesses and scar formation are seen in hidradenitis suppurativa
Another hypothesis is that there may be two subtypes of hidradenitis suppurativa, one in which the pathogenesis is that described above and another subtype that truly is a primary apocrine hidradenitis [89]. This view of the disease is not currently widely accepted.
10.9.3 Pathogenesis
Hidradenitis suppurativa is associated with follicular occlusion disorders , including acne conglobata, dissecting cellulitis of the scalp, and pilonidal sinus [90]. Histologic studies suggest that hyperkeratosis of the follicular epithelium may be the initial event in the disease process. The molecular basis of hidradenitis suppurativa involves loss of function mutations in gamma-secretase and defective Notch signaling . Notch signaling is important in the formation of epidermal cysts and in pro-inflammatory processes [91]. Gamma-secretase is a protein complex composed of four subunits encoded by separate genes, namely PSEN1/PSEN2, PSENEN, NCSTN, and APH1A/APH1B [92]. Gamma-secretase regulates Notch signaling by cleaving and activating intracellular Notch [93]. Mutations in the subunits of gamma-secretase have been identified in some patients with hidradenitis suppurativa [94, 95].
Immunological factors also contribute to the etiology of this disease. Increased levels of proinflammatory cytokines , such as tumor necrosis factor-α (TNF-α), interleukin (IL)-1β, and IL-17, have been identified in lesional skin [96, 97]. Bacterial colonization from follicular occlusion, and subsequent infection and inflammatory reaction are also contributing factors [98]. Smoking is another important factor in hidradenitis suppurativa . Patients with hidradenitis suppurativa have higher-than-average smoking rates [99, 100]. Smoking may promote follicular plugging and contribute to inflammation. Androgens and obesity may also play a role in this disease [101].
10.10 Alopecia Areata
10.10.1 Clinical Features
Alopecia areata may affect up to 0.2 % of the general population in the United States with a lifetime risk of 1.7 % [102]. Approximately 60 % of patients will have their first episode of hair loss before their 20th birthday with pediatric cases accounting for 20 % of the affected population [102]. Alopecia areata affects all races and ethnicities, and appears to have no gender predilection. Twenty percent of patients have a positive family history of disease [103].
The most commonly encountered phenotype is “patchy alopecia areata,” which is characterized by onset of asymptomatic, well-circumscribed, round to oval patches of non-scarring alopecia without scaling and occasional overlying subtly colored erythema (Figs. 10.17 and 10.18). Alopecia areata totalis is a subtype with complete loss of hair at the scalp, while alopecia areata universalis describes complete hair loss at the scalp and body. Ophiasis is a variant that portends a worse prognosis with hair loss in a band distribution along the periphery of the scalp. Diffuse and total alopecia areata is a newly-described entity with rapid onset of complete hair loss at the scalp over a 3-month period and eventual recovery of hair over 6 months [102].


Fig. 10.17
Alopecia areata is characterized by well-demarcated patches of non-scarring alopecia
Fig. 10.18
Exclamation point hairs in alopecia areata
Alopecia areata frequently waxes and wanes with most patients experiencing more than one episode of hair loss. However, approximately 50 % of patients with alopecia areata will have regrowth of hair and remission of disease within a year of onset [102]. Conversely, 5 % of affected individuals will have more severe disease with eventual progression to alopecia totalis or universalis. Patients with more generalized hair loss (alopecia totalis or universalis) have less than a 10 % chance of full recovery and hair growth [102]. Poor prognostic factors include the extent of hair loss at presentation, longer duration of hair loss, atopy, positive family history of disease, presence of other autoimmune diseases, nail involvement, and younger age at disease onset.
10.10.2 Histology
Most dermatopathologists view horizontal or transverse sectioning (Headington method) to be the optimal way to analyze alopecia biopsies, but others prefer the traditional vertical sectioning technique [104, 105]. Using either method, the histologic findings are the same, but are seen from different angles. A peri-bulbar and intrabulbar lymphohistiocytic infiltrate that is relatively mild is the commonest observation in early lesions (Fig. 10.19) [104]. Scattered eosinophils may be present in nearly half of all cases [106]. As lesions progress, there is a diminution in the size of hair follicles and a shift towards more telogen and catagen (best regarded as non-anagen) phase hairs [106, 107]. Fibrous tracts or “streamers” are often present in the deep dermis, representing hairs that have shifted towards an involution phase (Fig. 10.20). In these cases, pigment incontinence with melanin in melanophages is seen in and around the follicular bulbs. Pigment casts are also commonly encountered [106]. Increased numbers of vellus-like hairs are present in the subacute and chronic stages of alopecia areata [104]. There is no change in the density of pilosebaceous units, and no scarring or architectural alteration within the dermis.
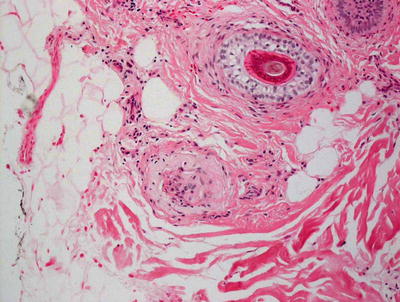
Fig. 10.19
The presence of a peri-bulbar lymphocytic infiltrate is a strong diagnostic criterion in alopecia areata
Fig. 10.20
Fibrous tracts representing residuum from follicles in catagen and telogen phase are seen with increased frequency in alopecia areata
Alopecia areata incognito is a variant of alopecia areata with a more diffuse pattern of hair loss. In these cases, there is no scarring, as is manifest in the normal density of pilosebaceous units. As in the more traditional variant of this condition, there is an increase in percentage of telogen phase hairs and increased vellus hairs. Follicular dilation is also described in this variant, while this is less commonly observed in the usual cases of alopecia areata [108].
10.10.3 Pathogenesis
The pathogenesis of alopecia areata has genetic and autoimmune contributions that are further modified by unknown environmental influences. There is a positive family history in 10–25 % of the cases of alopecia areata [109–111]. Monozygotic twins have a higher concordance rate (42 %) than heterozygotic twins (10 %) [111]. In a large study of 1054 patients and 3278 controls, 139 single-nucleotide polymorphisms (SNPs) related to the development of alopecia areata were identified [112]. From these findings, eight genes were found to be highly correlated with disease risk. Some of the disease “susceptibility loci ” appear to be important in autoimmune diseases, such as type 1 diabetes and rheumatoid arthritis.
Alopecia areata is a T lymphocyte-mediated autoimmune disease. CD8-positive T cells play a key role in disease pathogenesis [113, 114]. In alopecia areata, the hair follicles are primarily affected. There are autoreactive CD8-positive T cells present in the peribulbar region as well as in the follicular epithelium of the hair follicles, where T cells are thought to recognize auto-antigens presented by major histocompatibility complex class I [115]. The nature of the auto-antigens is not known. Attempts have been made to identify alopecia areata-specific intralesional CD8-positive T lymphocytes that might be the basis for specific immunotherapy [116].
10.11 Telogen Effluvium
10.11.1 Clinical Features
Telogen effluvium is a relatively common cause of hair loss, often occurring 3 to 6 months following an inciting event (typically life stressor, such as pregnancy, hospitalization, pronounced illness, or family death). The exact incidence is unknown [117]. Telogen effluvium is characterized by the relatively rapid onset of diffuse non-scarring, thinning of the scalp hair, including along the bi-temporal scalp (Fig. 10.21). Most patients do well with regrowth of hair within 6 to 12 months.

Fig. 10.21
Telogen effluvium is characterized by generalized hair shedding with clinically apparent decreased hair density
10.11.2 Histology
Histologic changes in telogen effluvium are subtle and most easily observed using horizontal sections to evaluate a larger number of hair follicles. The major finding is a phase shift with a disproportionate number of follicles in catagen or telogen phase, and a smaller number in anagen phase (Figs. 10.22 and 10.23). This shift is relatively slight and perhaps as many as 20 % (or double the normal number) of follicles will be non-anagen hairs. Due to this phase shift, biopsies demonstrate an increased number of fibrous tracts in the deepest portion of the dermis. Inflammation is rarely a feature of telogen effluvium and scar formation is not seen in this entity [118].
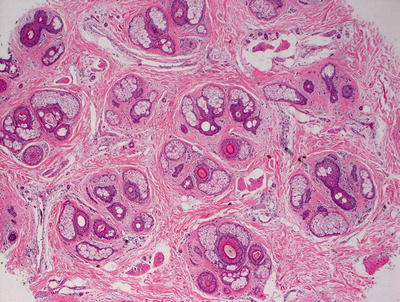
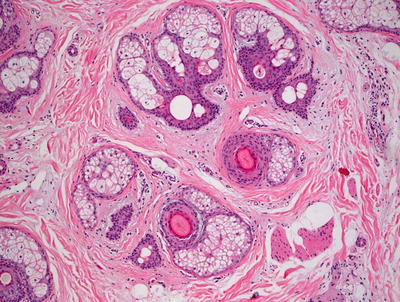
Fig. 10.22
Telogen effluvium is characterized by minimal inflammation and preservation of the pilosebaceous architecture with no scarring
Fig. 10.23
An increased percentage of hair follicles are present in the telogen phase in telogen effluvium
10.11.3 Pathogenesis
Telogen effluvium is a non-scarring alopecia, in which there is diffuse shedding of telogen hair [119, 120]. To establish the cause of telogen effluvium, relevant history and appropriate diagnostic studies to assess the endocrine and nutritional status, as well as potential autoimmune disorders of the patient are necessary. Hair follicles can shift from anagen (active proliferating phase) to telogen (resting phase) when exposed to stressors, such as infections, systemic illness, surgery, medication, and nutritional deficiency (such as proteins, iron, zinc, and essential fatty acids deficiencies) [117]. Iron deficiency appears to be important in telogen effluvium, because loss of iron reduces the proliferation of matrix cells. Iron deficiency without anemia is seen in 20 % of cases, and the only test indication is serum ferritin below 20 mg/l [121]. Changes in thyroid function, such as decreased thyroid hormone levels, can also result in telogen effluvium.
Telogen effluvium might be due to problems in hair cycle synchronization with shortening of the anagen phase. It has been proposed that hair follicles cycle to anagen phase within a few days, instead of staying in telogen phase for months as would be for normal hair [122]. Other studies also lend support to this “immediate telogen release” mechanism [123].
10.12 Anagen Effluvium
10.12.1 Clinical Features
Anagen effluvium is rapid loss of all terminal hairs in the anagen phase of hair growth. This condition most commonly occurs in patients receiving radiation or chemotherapy with incidence of about 65 % in chemotherapy patients [124]. There are reports of anagen effluvium following exposure to colchicine, boric acid, lead, thallium, arsenic, bismuth, and Coumadin [125]. The degree of hair thinning and subsequent hair loss is dependent upon exposure to the causative agent. Segmental thinning and narrowing may occur with low dose-exposure with hair pull tests yielding tapered “pencil point” hairs. Hair usually regrows once the causative agent is removed [124, 125].
10.12.2 Histology
The diagnosis of anagen effluvium is almost always made based upon clinical impressions and biopsies are rarely necessary in patients suffering from this condition. Cross-sectional analysis of skin biopsies reveals a non-scarring and noninflammatory process with normal number of anagen phase follicles, often lacking in hairs. There are no histomorphologic changes in the pilosebaceous units.
10.12.3 Pathogenesis
Anagen effluvium occurs when there is an abrupt loss of hairs in anagen (active growth) phase due to insults that impair the proliferative activity of the hair follicles. Examples of such insults include chemotherapy, radiation, toxic chemicals, and inflammatory diseases [126]. The anagen phase of hair growth has the highest proliferative activity. Acute damage of rapidly proliferating bulb matrix cells in this phase can result in failure of hair formation [127, 128]. About 90 % of hair in the scalp is in anagen phase. Therefore, loss of anagen hair can be copious with resulting alopecia. Proliferating bulb matrix cells are primarily affected in anagen effluvium, while quiescent stem cells of the follicular bulge are spared. Thus, anagen effluvium is reversible due to intact stem cell reservoir. The hair follicles typically resume the normal cell cycling pattern shortly after the cessation of events that disrupt hair growth [127–129].
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


