, Jane Tomimori1, Sofia Beatriz Machado de Mendonça1 and Douglas Antonio Rodrigues1
(1)
Universidade Federal de São Paulo, São Paulo, Brazil
5.1 Pityriasis Alba and Eczematid
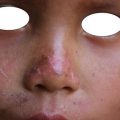
Pityriasis alba and eczematid are recurrent, noninfectious, and nontransmissible skin diseases of a constitutional nature. They are frequent among atopic (allergic) patients with dry skin. There is spontaneous remission, but recurrence is common. Eczematid may be considered an inflammatory form of pityriasis alba. It is a common disease, more frequent among children and young adults. Allergic people (with rhinitis or allergic bronchitis) are more likely to have the disease. Pityriasis alba is more clinically evident following sun exposure without sunscreen, which increases the contrast of the lesion against normal skin. Pityriasis alba shows white spots with fine scaling . This form affects the face (malar region), arms, and trunk (Figs. 5.1, 5.2, and 5.3) . It is asymptomatic. Eczematid is characterized by rounded erythematous-scaly lesions that can affect any part of the body but are more common in the trunk and limbs (Figs. 5.4 and 5.5) . This form is asymptomatic or can cause slight itching.





Fig. 5.1
Pityriasis alba: lesions on face
Fig. 5.2
Pityriasis alba: lesions on arm
Fig. 5.3
Pityriasis alba: lesions on face
Fig. 5.4
Eczematid: lesions on buttocks
Fig. 5.5
Eczematid: lesions on lower limbs
Diagnosis is clinical. In pityriasis alba, the histopathology shows a reduction in melanin and melanocytes in the basal layer of the epidermis. In eczematid, direct mycological examination is recommended if there is doubt about colonization by fungus.
The recommendations are to avoid prolonged exposure to the sun, take long baths, and to use soap extensively. The use of moisturizers is very useful for skin dryness control. In the case of pruritic lesions, the use of low-potency corticosteroids, such as 1% hydrocortisone cream, is recommended.
Frequently, indigenous populations are exposed to the sun, provoking a high contrast of pityriasis alba lesions and adjacent normal skin.
5.2 Contact Dermatitis
Contact dermatitis is an eczematous disease caused by contact with some substance that causes irritation or allergy in a given area. The patient may or may not have previous exposure to the substance (allergen).
The increase in chemicals has led to increased chances of developing contact dermatitis. This disease can affect anyone at any age, with or without prior exposure to the causative substance .
The lesions that arise in association with this disease are very itchy. When they are acute, vesicles or blisters are observed, accompanied by erythema and edema. Because they itch a lot, they are easily traumatized by scratching and become secretory. Chronic lesions are dry, and they are scaly with thicker and itchy skin. Lesions occur in areas where there was contact with the suspected substance (e.g., feet, hands, face) (Figs. 5.6, 5.7, and 5.8) . In allergic contact dermatitis, the lesions may reach other regions and become disseminated.



Fig. 5.6
Contact dermatitis: lesions on wrist
Fig. 5.7
Contact dermatitis: lesions on legs
Fig. 5.8
Contact dermatitis: lesions on legs
Once the suspect substance is identified, the patient should avoid any contact with or handling of the allergen. In acute cases, the use of topical corticosteroid (dexamethasone, betamethasone) until clinical improvement is recommended. The use of systemic antihistamines (dexchlorpheniramine, hydroxyzine, loratadine) can help to control the pruritus. In more severe cases, the use of systemic corticosteroids (injectable betamethasone, oral prednisone) is useful. In chronic cases, better results are obtained with a topical corticosteroid (betamethasone, clobetasol) as an ointment associated with oral antihistamine.
Indigenous populations have access to unknown and different substances. They can lead to various conditions of contact dermatitis as a primary irritant or allergic substance.
5.3 Seborrheic Dermatitis
Seborrheic dermatitis is a noninfectious and nontransmissible chronic skin disease . It is often associated with allergies (asthma, rhinitis, sinusitis, or eczema). On the scalp, the disease develops scales known as dandruff . There are many related factors such as fungal colonization (Malassezia spp.), sebaceous secretions, and emotional stress.
It is a disease with worldwide distribution and is frequent during the first 6 months of life and in adults after adolescence.
There are reddish (erythematous) lesions , with greasy scales, that can affect the scalp, face (eyebrow and nose region), chest, groin, and genital region (Figs. 5.9, 5.10, 5.11, and 5.12) . These lesions can cause local itching and inflammation. In young children (under 6 months of age) they can reach other areas of the skin as well (face, neck, trunk, and extremities). Often the formation of scales on the vertex of the scalp are observed, depending on the extent of the skin lesions. Mild forms are treated with topical azoles or ciclopirox olamine. Topical 1% hydrocortisone cream twice daily can be used until the inflammatory symptoms are under control. In adults with extensive lesions, betamethasone cream 0.1% twice daily is useful. The combination of ketoconazole, zinc pyrithione, selenium sulfide, or ciclopirox olamine shampoo may aid in treatment. The crusty mass on a baby’s scalp can be removed with sweet almond oil.




Fig. 5.9
Seborrheic dermatitis: lesions on scalp
Fig. 5.10
Seborrheic dermatitis: lesions on scalp
Fig. 5.11
Seborrheic dermatitis: lesions on genital region
Fig. 5.12
Seborrheic dermatitis: lesions on face
5.4 Neurodermatitis
Neurodermatitis is also called lichen simplex chronicus . It is a thickening of the skin resulting from chronic itching by different external stimuli, especially eczema or dermatitis (e.g., chronic contact dermatitis) and insect bites.
It afflicts people exposed to environmental conditions that lead to contact dermatitis, insect bites, or other chronic dermatoses. It affects anyone, especially elderly patients with dry skin. Emotional stress is another factor that can induce a pruritic sensation and scratching (Figs. 5.13, 5.14, and 5.15) .



Fig. 5.13
Neurodermatitis: lesions on leg
Fig. 5.14
Neurodermatitis: lesions on foot
Fig. 5.15
Neurodermatitis: lesions on leg
Thick, scaly, and hyperchromic plaques arise, showing accentuation of natural lines on the skin surface (lichenification). Pruritus is always present and may be mild, moderate, or very intense. Solitary or multiple lesions are observed on the posterior region of the neck and dorsum, in the anogenital region, and on extremities. Diagnosis is clinical. A skin biopsy may be necessary when there is diagnostic doubt. Examinations of the removed skin fragment are performed based on clinical suspicions (e.g., histopathological examination, cultures).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


