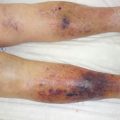
Fig. 12.1
A 66-year-old female, over years of medication of oral steroid (15 mg prednisolone) due to idiopathic thrombocytopenic purpura (ITP). Sudden onset of group A streptococcal necrotizing fasciitis in her right calf (right), ipsilateral thigh and inguinal lymph node inflammation (middle), and contralateral calf pigmentation largely due to ITP and continued hemorrhage (right)
Fig. 12.2
Severe tissue damage deep to the fascia by invading group A streptococci and host-releasing polymorphonuclear (PMN) leukocytes (arrows)
12.5 Diagnosis and Tests
12.5.1 Physical Diagnosis
The odds ratios (OR) of fever, tachycardia, and hypotension between necrotizing fasciitis and non-severe soft tissue infection are 3.4 (1.6–7.4), 4.5 (1.7–11.8), and 2.6 (1.1–6.0), respectively [7]. The likelihood of the presence of bullae in NF in comparison to non-severe soft tissue infection is 3.5 (1.0–11.9). Skin necrosis is present in 6 % of NF and in 2 % of non-severe soft tissue infections. At first, physical findings of NF include erythematous and ecchymotic skin lesions, and these rapidly evolve into bleeding bullae, indicating occlusion of deep blood vessels in the fascia or muscle compartments; thus, the presence of the bullae is crucial for clinical diagnosis. Ludwig’s angina (submandibular space) and Fournier’s gangrene (scrotum and penis or vulva) are variant forms of NF and often demonstrate explosive and aggressive clinical courses.
12.5.2 Laboratory Tests
The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score is developed expecting diagnostic clues for NF. Among the total 13 scores, retrospective study suggests that a score of 6 and more is highly indicative of NF with 92 % positive predictive value and 96 % negative predictive value [8]. LRINEC score is helpful in categorizing patients into risk factors of NF.
12.6 Treatment
12.6.1 Medical Therapy
Suspected NF patients should be empirically and immediately administered with broad-spectrum antibiotics, which may cover the common suspected pathogens. The first-line antimicrobial agents to necrotizing fasciitis are depicted in Table 12.1. In type I (polymicrobial) infection, the selection of an antimicrobial should be based on medical history and Gram staining and culture. The coverage against anaerobes is important in type I. Metronidazole, clindamycin, or beta-lactams with beta-lactamase inhibitor or carbapenems are of choice against anaerobes. In patients already exposed to antibiotics in advance, broader Gram-negative coverage should be taken into account for an initial empirical therapy. Ampicillin-sulbactam, piperacillin-tazobactam, ticarcillin-clavulanate, newly generated cephalosporins, or carbapenems are the candidates for this purpose. In type II (monomicrobial), the most causative pathogen is group A streptococcus, but sometimes Methicillin-Susceptible Staphylococcus Aureus (MSSA)/Methicillin-resistant Staphylococcus Aureus (MRSA) The use of tetracyclines and third-generation cephalosporins is crucial to managing Vibrio infection. The systemic antibiotic therapy for NF may continue 4–6 weeks as the deep-seeded infection is established. Intravenous immunoglobulin (IVIG) is a desirable option to neutralize streptococcal toxins.
Table 12.1
Treatment of necrotizing fasciitis, first-line antimicrobial agent
Mixed infection | Streptococcus infection |
Ampicillin-subactam | Penicillin
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|