(1)
Division of Plastic-, Hand-, and Microsurgery Department of Surgery, Ludwig Maximilians University, Munich, Germany
3.1 Indication and Prerequisites
Circumscribed impairment of the lymphatic system is the main indication for lymphatic grafting. In most cases, such a blockage results from surgical interventions such as lymphadenectomies in the axilla, groin, or pelvic area. Also dissections of lymphatic trunks in narrow parts of the lymphatic system, e.g., on the medial aspect of the knee, may lead to a lymphatic obstruction. In addition, infection or radiotherapy often damages the lymphatic pathways additionally and leads to the clinical manifestation of lymphedema.
A further indication exists for special forms of primary lymphedema with a regionally compromised lymphatic pathway, e.g., a unilateral lymphatic atresia at the groin and pelvis (Kinmonth 1982).
The following requirements have to be fulfilled prior to surgical treatment of secondary lymphedema (Table 3.1):
Table 3.1
Indication and prerequisites for lymphatic grafting
1. Circumscribed interruption or impediment of lymphatic flow |
2. Undisturbed lymphatic system at least in one leg for harvesting |
3. Lymphatic channels with a lumen at both sides of diseased area |
4. Free of recurrence of malignant diseases |
5. Capable for general anesthesia |
6. Microsurgeon, experienced in microsurgery and lymphology as well |
It is recommended to keep an interval of at least 6 months after the surgery or intervention, which has been followed by transitory swelling due to the interference with the lymphatic system. During that period of time, spontaneous normalization might occur, and lymphatic grafting may become superfluous. This time period should be used by complete decongestive therapy (CDT) which consists of manual lymph drainage, compression therapy, and exercises combined with skin protection.
After tumor therapy, an exact evaluation of the patient with respect to possible recurrence of the tumor is necessary.
In order to perform autologous lymphatic grafting, the harvest from the patient’s thigh must be possible respecting residual lymphatic transport capacity after removal of the graft.
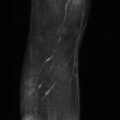
A preoperative lymphoscintigraphy permits evaluation of the lymphatic transport capacity in the donor region. If lymphatic flow is impaired in the donor region or there is swelling in the same region, lymphatic vessels should not be harvested.
The most important prerequisite is however the microsurgeon. He should have an extensive practice in microsurgery. Normally this deals however with vessels of more than 2 mm in diameter. Dealing with structures of less than 0.3 mm needs a considerable additional effort and therefore additional training.
The understanding and knowledge of lymphology is another prerequisite in order to avoid to be only a worker in a highly demanding manual field. The investigation of the patient, the appropriate indication, and the knowledge of managing complications and further possible treatment options need a profound expertise in the field of lymphatic diseases.
3.2 Equipment
The most advanced available microsurgical equipment should be used in order to facilitate the microsurgical demanding surgery on lymphatic vessels.
The microsurgeon should take advantage from the possible support to allow him just to move his hands and to get support for his forearms and elbows. Sometimes also breathing may be disturbing. It is advisable not to stop it with exertion, but to incorporate such periods within the workflow and repeat them more often instead of pausing for a longer time (Fig. 3.1).

Fig. 3.1
Microsurgeon sitting in a chair with suspended forearms, operating microscope, ultrafine microinstruments
The operating microscope is critical. It should allow high magnification of up to about 40-fold.
Improvements might be seen with addition of near-infrared light source allowing indocyanine green investigations during the surgery. However the visibility of lymphatic vessels is limited to the superficial area of the subcutaneous tissue. Therefore, the main lymphatic collectors which are located above the deep fascia may not be detected.
In order to manipulate the delicate lymphatic vessels, the finest microsurgical instruments available should be used. The tips of the pincers should measure not more than 0.1 mm.
Also the suture material should be adapted to the size of the vessels to be anastomosed. In our personal experience in animals, we had the impression that reducing the foreign body reaction might be of advantage, looking at the histological findings showing large particles of the suture material next to the anastomoses. Since the production of polyglactin 910 (Vicryl®, Ethicon) with the size of 11-0 has been stopped, we use the remaining 10-0 (Baumeister et al. 1982).
However, nonabsorbable suture material, which is tinier than 12.0, might reduce the unfavorable correlation between vessel diameter and foreign body reaction.
Regarding the type of the needles, round needles are enough to penetrate the lymphatic vessel wall. For absorbable suture material, the smallest available needle size at the moment is BV 75-4.
To facilitate the suturing and handling the lymphatic vessels, a green plastic sheet is put underneath the vessels. Addition of some drops of Ringer’s solution mixed with heparin helps to discriminate the front and back vessel walls by suspending the vessels.
3.3 Basic Technique
The basic technique follows the principles of vascular surgery and the adjustment to the special needs of lymphatic vessels. Elements were developed during the experimental phase of the reconstructive microsurgery of lymphatic vessels (Baumeister et al. 1981b, 1990, 2003).
3.3.1 Discriminating Lymphatic Vessels
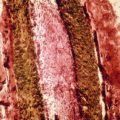
Looking for lymphatic vessels is easy if they got stained. For staining, the dye has to get almost exclusively to the lymphatic system. This means that the molecular weight is relatively high in order to be ingested exclusively into the lymphatic capillaries. In Europe, Patent Blue V® is used for these purposes and fulfills these prerequisites (Fig. 3.2). The dye should be administered close to the subdermal lymphatic plexus. Thereafter it is quickly incorporated within the lymphatic system. Passive movements in anesthetized patients alleviate the transport to the base of the extremity within several minutes.
Fig. 3.2
Lymphatic collectors stained with Patent Blue V®
To search lymphatic vessels, a superficial incision just of the skin and dermis is recommended. By that way superficial tiny lymphatic vessels will not be harmed. Middle-sized lymphatic vessels in the subcutaneous tissue are located just within the adipose tissue or adjacent to major veins. The biggest lymphatic collectors are found mostly close to the deep fascia.
Underneath the fascia bigger lymphatic vessels can be found between the main arteries and veins.
Within the subcutaneous tissue, gently spreading movements in an oblique fashion to the main direction of the lymphatic vessels with a bigger instrument—I am using the “Metzenbaum” scissors—allow access to the stained lymphatic vessels. At the start of searching, one should try to get an overview of the vessels present in the corresponding area, e.g., the ventromedial bundle at the thigh. The surrounding tissue is separated from the lymphatic vessels. These are not touched until their course became obvious. Only prior to the harvest, the fine preparation starts. Intact bigger lymphatic collectors are relatively resistant against longitudinal tension. They can be elevated by fine hooks or also gently elevated by wet fingers.
In the edematous tissue, the lymphatic vessels do not get stained like in an undisturbed lymphatic flow. Therefore, we do not attempt to perform a staining like we do during the harvesting process. Therefore it is difficult to discriminate between small veins, small nerves, fibrous bands, and the altered lymphatic collectors. Since the area of search is limited and is performed in oblique direction, only a limited number of structures have to be checked.
The lymphatic collectors are mostly somewhat hidden within the subcutaneous tissue. The biggest ones are located just above the deep fascia. Lymphatic collectors are gray shining and are often separated from the surrounding adipose tissue. Small nerves instead have a bright white appearance and show oblique silver-shining stripes. The final decision sometimes can only be made after transection of the structure. Veins deliver blood. Out of the nerves prolapses the axon. A lymphatic collector should show a lumen without blood, preferentially delivering clear fluid.
In the treatment of a lymphocele, staining of the incoming lymphatic vessels is mostly possible. Blunt dissection of the distal part of the lymphocele directs to the incoming vessels. If fibrous tissue hinders the dissection from the outside, the lymphocele can be opened. The holes in the wall at the distal area, together with extrusion of stained fluid, will clarify the source of the lymphocele.
3.3.2 End-to-End Anastomosis
The two lymphatic vessels should be situated next to each other.
The first stitch is the most difficult one since the wall is collapsed. It might be helpful to add a small amount of Ringer’s solution mixed with heparin helping to lift the wall (Fig. 3.3). In very small lymphatic vessels with fibrosis around the lumen, it might be advisable to only fix the outer layer with the stitches. The content of the lumen of the vessel can then drain into the graft.
Fig. 3.3
End-to-end anastomosis, first corner stitch. Graft with translucent wall above, sclerosed lymphatic vessel of lymphedematous tissue with the lumen surrounded by fibrosed wall below (© Baumeister)
The back wall is just lifted when starting to anastomose. The first stitch is placed at the far end of the vessels.
The sutures are directed from outside to inside and back on the opposite wall.
The second corner stitch is placed in front of the surgeon.
The suture is finished with the closure of the front wall.
Care should always be taken to avoid tension to the lymphatic vessel wall in oblique direction.
In longitudinal direction the vessel as a whole is however remarkable resistant against tension.
The number of stitches is dependent on the size of the lymphatic and the condition of the vessel wall.
Very small lymphatic vessels may just be adapted by one single stitch.
Danese (1982) had shown experimentally that lymphatic collectors may perform anastomosis by themselves if they come close to each other. This is encouraging for the microsurgeon. He will learn to minimize the disturbance for the lymphatic vessel.
In middle-sized lymphatic vessels, three to four stitches are enough.
Leakage will not be a problem since the pressure is low (Fig. 3.4).
Fig. 3.4
End-to-end anastomosis completed. Graft filled with lymph (© Baumeister)
In big or enlarged lymphatic vessels, around 6 to 8 stitches can be applied.
The graft is filled with lymph at the end of the anastomosis also when the wall of the lymphatic vessel within the edematous tissue shows fibrosis (Fig. 3.5).
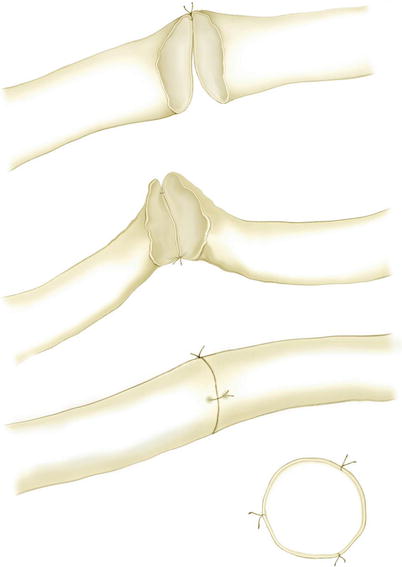
Fig. 3.5
End-to-end anastomosis with three stitches (© Baumeister)
Different reason may contribute to this phenomenon.
A lumen can be seen also in lymphatic collectors in severe and long-standing lymphedemas.
Reconstruction within the lymphatic system does not need a pressure to work against another system like in lympho-venous anastomoses.
Lymphatic vessels are known for the active transport of the lymph. Lymphatic vessels continue pumping also in nutrient solution.
We saw recovery of activity along the lymphatic channels which was not present prior to the grafting in lymphedema patients in follow-up lymphoscintigraphies.
Therefore, a suction force produced by the lymphatic grafts can be postulated which helps to empty lymphatic vessels, also when they are not able to pump themselves.
Related posts:
 Reconstructive Lymph Vascular Surgery and Other Lymphedema Treatment Modalities
Reconstructive Lymph Vascular Surgery and Other Lymphedema Treatment Modalities
 Pathophysiology of Lymphedemas with Respect to Surgery
Pathophysiology of Lymphedemas with Respect to Surgery
 Methods for Objectification of the Results
Methods for Objectification of the Results
 Experimental Basis of Reconstructive Lymph Vascular Surgery
Experimental Basis of Reconstructive Lymph Vascular Surgery
 Results of Reconstructive Lymph Vascular Surgery
Results of Reconstructive Lymph Vascular Surgery
 Pityriasis alba
Pityriasis alba
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


