Chapter 3 Implant Basics
There are many factors that combine to determine the quality of the aesthetic result obtained when an implant is placed under the breast. Some of these factors are relatively fixed and are therefore subject to limited control by the surgeon. Perhaps the most important variable that falls into this category is the nature of the pre-existing soft tissue framework of the breast. However, one variable that is most decidedly under the control of the surgeon is the nature of the implant that is chosen to perform the procedure. By intelligently choosing the correct combination of implant characteristics, the results obtained after breast augmentation can be optimized as much as possible. Therefore, while other decisions that are made when planning a breast augmentation such as incision location and pocket placement are without question of great importance, choosing the ‘right’ breast implant is one of the most critical decisions to be made in breast augmentation.
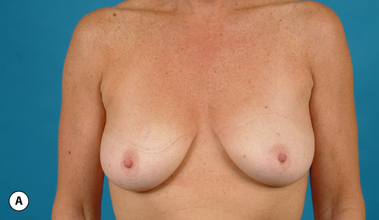
It bears emphasizing that the effect of the implant on the ultimate result after breast augmentation is directly related to the thickness of the soft tissue cover of the breast. In patients where there is a relatively thick layer of parenchyma and fat, essentially any breast implant will provide an acceptable result if the proper volume is provided. There is no reason to use, for instance, a shaped device in these patients as the advantage of the anatomic shape is overwhelmed by the volume of the surrounding soft tissue and the subtleties of the shaped concept are so obscured as to be rendered inconsequential. In fact, when the volume of the breast implant ends up providing 50% or less of the overall volume of the breast, any shaping advantage afforded by an anatomic device, or any more subtle ‘feel’ effect associated with, for instance, a silicone gel implant, ends up being obscured by the volume of the native breast. As the percentage of overall breast volume that the implant provides increases, the effect that the shape, size and consistency of the chosen breast implant has on the final result becomes more pronounced. Generally speaking, when the implant provides more than 75% of the volume of the breast, variables such as shape, fill material and projection begin to have an increasingly noticeable effect on the overall result (Figures 3.1, 3.2).







Implant Construction
The outer shell is made of a silicone rubber that is cured onto a form called a mandril. The mandril is specifically constructed to create an implant of a specific size and shape. For a given implant design, there are generally whole families of mandrils which maintain the basic shape but exhibit a wide range of graduated dimensions and volumes. Either the mandrils are dipped into liquid silicone or the silicone is sprayed on to apply a thin coat of the material to the mandril. This thin layer of liquid silicone is allowed to dry and the mandril is then dipped again. After a series of dips, the silicone layer that is now attached to the mandril has a uniform thickness sufficient to hold reliably a given volume, the configuration of which is determined by the shape and dimensions of the mandril that made the shell. The flexible silicone shell is cut free from the dipping rod attached to the mandril and the elastic form is stretched and pulled off. For saline implants, the circular defect created by freeing the shell from the mandril is patched and a small fill valve is inset into the patch to complete the construction of the shell. For silicone gel implants, the shell is filled with a prescribed volume of the chosen gel and the defect is then patched to seal the gel inside the shell (Figure 3.3 A–E).




Implant Behavior
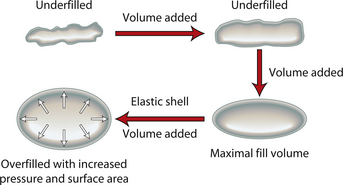
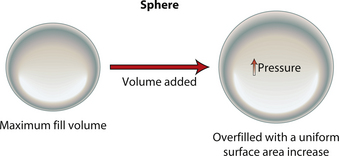
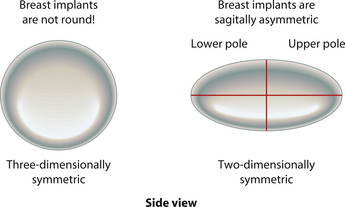
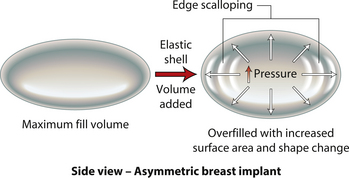
When an implant shell is completely empty, the outer shell is wrinkled and the shape of the device is correspondingly distorted. As volume is added to the implant, the wrinkles are filled out and the shape progressively improves until, eventually, a volume is reached where the shell is completely filled and, without any other outside influences, the shape of the implant exactly approximates the shape of the mandril that made the device. However, because the outer silicone rubber shell is elastic, it is possible to continue to fill the implant to a point beyond the fill volume determined by the mandril. As a result, the surface area of the implant expands slightly and the intraluminal pressure of the device increases (Figure 3.4). It is at this point that the physics-based relationships between surface area and volume become important. Very simply, for a given volume, the smallest surface area that can contain that volume assumes the shape of a sphere. Put another way, a sphere describes a surface area to volume relationship that is maximally efficient. This explains why breast implants appear rounded when they are subjected to the forces of capsular contracture. Because the volume of the device is fixed, as the surface area of the capsule decreases due to the contracture, the relationship between the surface area of the capsule and the volume of the implant becomes more efficient and gradually assumes the shape of a sphere (Figure 3.5 A,B). Therefore, with a perfectly spherical implant shell, overfilling would result in an increased intraluminal pressure and a symmetrically realized increase in the surface area of the implant with no distortion in the shape of the device (Figure 3.6). Essentially, all that would result would be a slightly bigger sphere that felt a little firmer. However, breast implants are not spherical in shape and it is very important to realize that what are commonly referred to as round implants are round only in two dimensions. Typically, in the horizontal and vertical planes, the devices are symmetric. However, in the sagittal plane, the dimensions of the implant are different and, in that regard, what is typically referred to as a round implant is actually shaped (Figure 3.7). Although this typical ‘round’ implant does not approach the degree of shape that the more standard ‘anatomical’ implant does, it is shaped nonetheless as it has asymmetrical dimensions in one plane and therefore functions as an asymmetric device. This asymmetry in shell design has implications in how the implant responds to filling. As the implant proceeds from an empty state to one of progressive inflation, the shape will improve until that point is reached where the exact volume that corresponds to that of the mandril is reached. This is the optimal fill volume for the implant. As this optimal fill volume is exceeded and the implant becomes overfilled, the surface area of the device increases slightly and the pressure inside the device increases. As continued filling proceeds, the ability of the outer shell to stretch to accommodate the increasing volume becomes overwhelmed and the increase in the surface area of the implant tails off rapidly such that the surface area measurement becomes more or less fixed. At this point, the laws of surface area to volume physics become applied and the device gradually becomes more spherical and the projection in the sagittal plane increases and the vertical height and horizontal width diminish. Because the contour of the radius of the device is more aggressively shaped as compared to the smoother dome-like contour of the front and back of the implant, the ability of the elastomer in this part of the shell to stretch smoothly to re-accommodate the increasing volume of the implant is limited. Therefore, as the projection of the implant increases, the change in the shape of the device cannot be smoothly accommodated along the radius of the device and stress risers form at the implant edge. This is a well-recognized phenomenon noted particularly in saline implants and this edge distortion is known as ‘scalloping’ (Figures 3.8–3.10, (uDVD clip 1.05)). As the implant is overfilled even further and becomes more spherical, the edge scalloping becomes more severe. Recalling the example of capsular contracture, where the volume remains fixed and the surface area gradually decreases, here in the case of an overfilled implant, it is the surface area which becomes more or less fixed and the volume which increases. In either instance, it is the physics of adding of fluid to a confined space that ultimately governs the resulting shape of a breast implant.


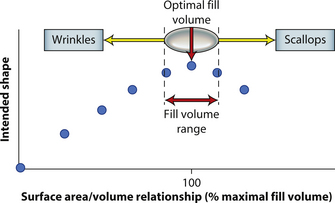
By applying these concepts, it is possible to gain a better understanding of implant behavior with regard to, in particular, saline implants. Figure 3.11 represents a stylized graph showing implant shape on the Y axis and degree of implant fill on the X axis. Initially, the implant is empty and the shape is an unfilled shell. Then, as fluid is added to the device, the wrinkles in the device are filled out and the shape gradually improves until the optimal fill volume, or the fill volume determined by the implant mandril, is reached. As further filling proceeds, scallops develop at the edge of the implant and the shape begins to deteriorate. Therefore, with the optimal fill volume as the apex of the desired shape, there is a small window of fill volume variability either side of which will still allow an acceptable shape to be created in the implant. Falling too far short of the optimal fill volume will result in progressively prominent wrinkling in the shell and exceeding the optimal fill volume by too great a degree will result in scalloping of the implant edge (Figure 3.11). This fill volume window has long been recognized by plastic surgeons and manufacturers and it is generally accepted that the optimal fill volume of a saline implant can be exceeded by roughly 10% without creating an obvious shape distortion. Such flexibility in implant filling is one of the advantages afforded by the use of saline implants. By differentially filling an implant of the same basic size and dimension without causing a significant distortion in the shape of the device, patients who present with mild asymmetries in breast size can be treated effectively without the potentially troubling need to resort to implants of different base diameters.
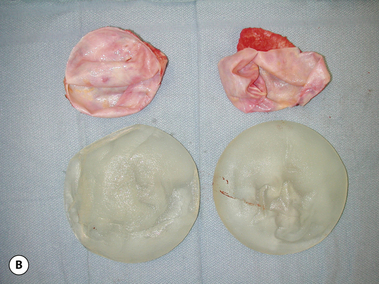
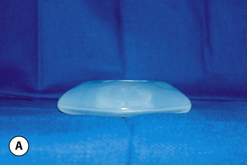
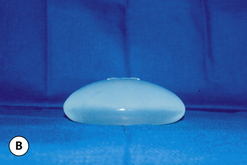
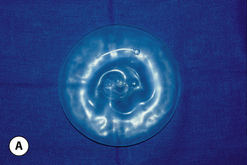
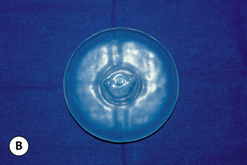
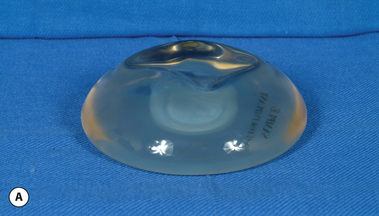
These principles are equally applicable to ‘round’ silicone gel implants. However, when comparing the characteristics of saline versus silicone gel implants, it is important to recognize two major differences. First, the volume of a silicone gel implant is fixed, a feature that actually simplifies the use of these devices to a certain extent. Second, every silicone gel implant, whether it be a moderate-, moderate plus- or high-profile device, is underfilled relative to the optimal implant volume created by the mandril. This mismatch in fill volume relative to the available surface area of the device, along with the thicker consistency of the gel, results in an implant which has a decidedly softer feel than a properly filled saline implant. When a silicone gel implant is placed on a flat surface, the degree to which it is underfilled can be assessed by noting the variable degree of collapse of the central part of the shell in the middle of the device (Figure 3.12 A,B). This central shell collapse can be temporarily corrected by gently placing an evenly applied force to the surface of the implant. The implant then assumes a properly filled appearance without deformation. A similar phenomenon occurs when the implant is placed upright 90 degrees. The underfilled device will collapse in the upper pole, sometimes markedly, and this collapse can be partially overcome by applying force to the anterior surface of the device (Figure 3.13 A,B). In situ, this external force is applied to the implant by the surrounding soft tissue framework of the breast. Therefore, the outward appearance of a breast augmented with an underfilled fixed-volume silicone gel implant will depend upon the degree of underfilling of the device as modified by the nature of the external forces applied by the soft tissue framework of the breast.



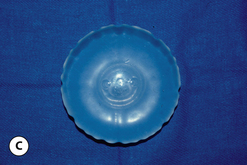
Given these variables, it can be deduced that saline-filled devices must be filled to a level at or near the optimal fill volume of the device lest the resulting surface irregularities which would develop, either wrinkles or scallops, become visible through the breast. These surface irregularities become even more pronounced when what appears to be a properly filled saline implant is placed upright 90 degrees. In this position, the pressure of the saline falling to the lower pole of the breast creates collapse of the upper pole with pronounced folding and wrinkling being the result (Figure 3.14). Applying force to the surface of the device, as happens with a relatively constricted soft tissue envelope, will counteract the tendency for the saline to fall to the bottom of the shell and upper pole distortion will tend to be corrected. However, in a lax skin envelope, if the soft tissue cover is thin enough, these irregularities develop unchecked and implant distortion with visible contour irregularities in the breast can potentially be seen. Silicone gel implants are under less severe constraints and can be underfilled without causing the same degree of potential surface irregularity. This is due to the fact that the denser consistency of the gel and the softer elasticity of a silicone gel implant shell combine to form softer wrinkles, which create edges which are less sharp than in saline devices. As a result, a fixed-volume, underfilled, silicone gel implant can settle to the bottom of a breast pocket and can fold and wrinkle according to the dictates of the overlying soft tissue framework to assume a shape other than that imparted to the shell by the shape of the mandril. Simply stated, the wrinkles associated with a standard round silicone gel implant tend to be much softer than those which form in saline devices and result in visible surface irregularities only in the thinnest of patients. In actuality, this shape is variably and at times markedly anatomical, a fact which has been documented in supine, prone and most importantly upright magnetic resonance imaging (MRI) evaluations of patients with fixed-volume silicone gel implants in place (Figure 3.15 A–G





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


