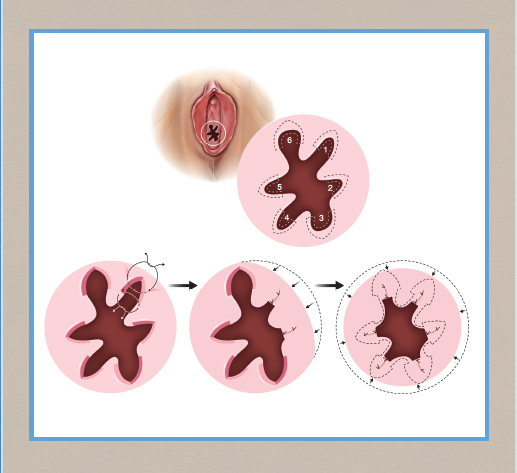
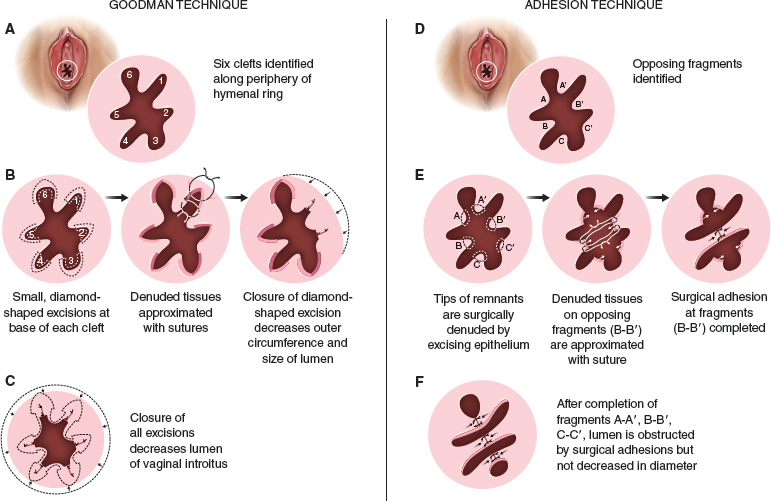
CHAPTER 12 • Hymenoplasty is the most secretive and least studied aesthetic female genital surgery procedure. • Information about the procedure tends to be based on anecdotal reports. • Hymenoplasty has numerous ethical issues. • Sociocultural factors play a major role. • Most indications for hymenoplasty are ritualistic versus aesthetic. • Establishing goals of the procedure with each patient is essential. • Follow-up after hymenoplasty usually does not occur. • Preoperative counseling may reduce surgical rates by 75%.1 Hymenoplasty, which is also referred to as hymenorrhaphy, hymen reconstruction, hymen repair, hymen restoration, hymen surgery, and revirgination, is the most popular term describing surgery to reestablish the integrity of the hymen and will be used in this chapter. Of all the aesthetic female genital procedures, hymenoplasty is mired in controversy and secrecy. Although it has been classified by the World Health Organization as a type of female genital mutilation, it now is generally considered distinctly different.2–5 Hymenoplasty is typically performed as an elective procedure; however, classifying it as an aesthetic procedure could be misleading, because others consider it more reconstructive, although nonfunctional, in nature. Although opinions about the nature of the procedure abound, few articles discuss technical details, and data are insufficient to provide evidence to support or recommend an effective surgical approach. Patient follow-up rarely occurs, because the intended results are transient and patients prefer anonymity postoperatively.6,7 Therefore many of the comments reported here were acquired on a personal basis during patient interactions and otherwise cannot be substantiated using traditional medical references. It has been said that, “A woman’s future can hang, literally, by a membrane.”8 Although patient safety is paramount, debate over the medical risks and practitioner skills are countered by fears of social ostracism and/or physical harm.5,9 Central to this discussion is whether hymenoplasty should be performed at all, which essentially is a matter of ethical deliberation.10 The approach to hymenoplasty depends on the respective culture and the value it places on virginity.3,11 Among university students in Turkey, a recent survey demonstrated the persistence of a double standard for male versus female attitudes for the traditional value of virginity that drives the demand for hymenoplasty.12 Although many assume hymenoplasty is more popular in Islamic cultures, the procedure has been performed in other cultures around the world. For example, an estimated 2% of women in Guatemala may have received this operation, often by practitioners with questionable training and a lack of monitoring or oversight.13 Hymenoplasty is the most secretive and least studied aesthetic female genital surgery procedure. Information about the procedure tends to be based on anecdotal reports. The influence of religion, traditional customs, and personal beliefs may also be reflected in a particular society’s legal codes.9,14 In these countries, practitioners will offer the procedure out of a moral obligation for the safety of women requesting it, despite personal ethical reservations and the risk of punitive consequences.15 Although the definition of virginity may be contested, many people consider an intact hymen to be the sine qua non of sexual chastity.16 For many cultures, the presence of an unbroken hymen is consistent with moral behavior and an indication of honor and integrity. I have been told stories of (1) mandatory physical examinations by “qualified” practitioners before the marriage ceremony, (2) a required breaking of an intact hymen with a cotton/silk cloth wrapped around the inspector’s index finger, (3) the mother-in-law being present at the time of consummation, and (4) the proud display of the bloody sheet. In Turkey, nearly any individual with a “vested” interest can demand a hymen examination as confirmation of virginity.17 Historically, major religions (Christianity, Judaism, Islam, Buddhism, and Hinduism) associate sexual abstinence with moral purity, and sexual activity is condoned between married individuals. Women who have had or even are suspected of premarital sexual activity (as evidenced by a compromised hymen assessed using a variety of methods that vary on a cultural basis) may be subjected to cancellation of marriage vows, public humiliation, excommunication, banishment, physical abuse, or other legal repercussions, including sentencing to capital punishment, imprisonment, or death (honor killing).9,18,19 One report arguing for repair stated the Egyptian practice of hymenoplasty actually reduced the frequency of “cleansing” murders by 80% compared with the previous decade.9 The ethics committees of multiple international medical societies (United States, United Kingdom, France, Canada, New Zealand, Australia, and the World Health Organization) have generally incorporated hymenoplasty as a genital cosmetic procedure.19–21 Goodman et al22 have proposed the four ethical principles (patient autonomy, nonmaleficence, beneficence, and justice) that distinguish elective vulvar plastic surgery from genital cutting practices. Ethicists support physicians’ decisions to perform surgery to protect women from adverse consequences.23 Conversely, others suggest, “Gynecologists with sufficient skills asked to perform the procedure should ethically take into account the consequences of their refusal.”5 Kopelman24 advised institution of the “Best Interests Standard” when weighing the decision to perform a hymenoplasty but thought this to be secondary to the “growing problem of forced marriages.” Earp25 suggested that physicians charge the “lowest possible fee” while combatting the greater social structure that drives the demand. Some propose that the availability of the procedure exposes a more troublesome incidence of sexual abuse, vulnerability to sexual harassment, and lack of appropriate sexual education.14 Critics of the procedure think it can become obsolete if the public learns to accept that bleeding or hymenal examination or certificates are not confirmations of virtue.19 Advocates have advanced elegant arguments for scientific evaluation of hymenoplasty practices and a multidisciplinary team of “surgeons, lawyers, social activists, champions of human rights, and religious leaders” to establish a solution to the controversy.18,26 Rarely, I have been asked to perform an elective hymenoplasty by both partners to comply with this marriage ritual or, even more rarely, to celebrate a second honeymoon. However, it is more often requested by a female, with or without accompanying family members, to conceal any history of premarital sex from an intended future partner and to ensure the perception of virginity. This is desperately sought after to prevent the dire consequences discussed previously. The same ethical issues discussed previously apply. Within this context, many practitioners, including male and female plastic surgeons, refuse to participate in a surgical procedure that (1) is not medically necessary, (2) holds women (versus men) to a higher standard of premarital abstinence, and (3) perpetuates deception of an unknowing victim: the sexual partner.5,7,27 One author argues that even if the bridegroom is aware, then the physician is colluding with deceit of other family members. Others question these moral arguments, given plastic surgeons’ performance of breast augmentation and liposuction. These operations are similarly not disclosed to partners and are also intended to present a facsimile of a natural physical state.22 Some think that hymenoplasty, unlike purely cosmetic procedures such as breast augmentation, may serve a “more worthy and protective” purpose.7 In some cultures, a “certificate of virginity” may be demanded on completion of the procedure; surgeons must be prepared to manage and address this moral conflict and their complicity in the deceit.28 Ethicists have justified the need to provide these certificates for patients at great risk of harm to their “well-being, autonomy, or personal integrity.”29 The embarrassment of being subjected to a physical examination (for the purpose of being “officially certified” as a virgin) has caused a number of women to commit suicide.17,19 This has prompted some advocates to suggest that partial monetary coverage should be made available when the indication is not purely aesthetic.7 Proponents think that the confidentiality of the doctor-patient relationship and the woman’s request supersede all other concerns.14 Others object on the basis that this maintains a prejudiced societal standard of virginity to which only women are held. Therefore condoning surgery preserves a myth that an intact hymen is a symbol of virginity. Some argue that eliminating these preconceived notions may not be a medical or legal issue and requires more of a social structural change.17,23 Others describe it as a “ritualistic surgery” that equates with circumcision and correlate the ethics with those of cosmetic surgery.14,18,30 The function of the hymen is unknown but has been proposed as a vaginal barrier against external sources of infection until puberty.31 Some have stated that there is, “no valid scientific indication” for hymenoplasty,18 and that it is performed primarily for cultural indications.8 Nearly anyone who presents with realistic expectations and has sufficient tissue to approximate is a candidate for elective hymenoplasty. Variations in technique can be performed for patients with insufficient hymenal fragments (Fig. 12-1). The timing of anticipated coitus may play a role in selecting a surgical approach and is discussed later in the chapter. Critics of the procedure claim unscrupulous surgeons may not provide proper information to patients and encourage patients to undergo the procedure to benefit from financial incentives.13,18 Fig. 12-1 In the examination room it is difficult to see hymenal fragments (*). Although screening methods have been recommended for patients undergoing female genital plastic surgery, no established tools exist for evaluating hymenoplasty candidates.22 The rapid healing of hymenal injuries may result in very little evidence of damage.32 The hymen has no standard appearance; a wide variety of anatomic variations have been described.8,33–37 Normal variations may occur with advancing age, and the hymenal morphology may change.37–40 Studies have shown a high incidence of nonspecific findings in hymenal morphology among women without a history of sexual abuse.41 Moreover, the optimal hymenal diameter or size has not been determined.42,43 Studies and discussions for establishing the “ideal” hymenal width and/or transhymenal diameter are inconclusive and summarized in an article discussing hymenal findings in females with and without a history of sexual abuse.44 Thus, there is no standard hymenal appearance to reproduce or reconstruct. Patients should be informed about the procedure with a thorough review of the risks, alternatives, and benefits consistent with the principles of informed consent. When discussing the role and goals of the procedure, surgeons should discuss the following topics: • Repair has no direct medical beneft.18 • Absence of the hymen or failure to bleed is not necessarily a sign of previous intercourse.19 • Less than half of the women in a retrospective survey stated they had not bled with initial sexual penetration.45 In a study from Amsterdam, 75% of counseled women elected not to proceed with hymenoplasty.1 They were informed that despite expressing a desire for postcoital bleeding and assurances that they would be sufficiently “tight” on their wedding night, surgery could not guarantee either. Bleeding on first coitus does not necessarily indicate virginity, and in a survey of 41 women, only 34% of the virgins bled on first intercourse, and 63% did not.14,46 Determining on physical examination whether a patient has had prior sexual activity is not always possible.47 In one study where ease of speculum examination was assessed, it was judged to be easily inserted in 56% of women who had denied sexual intercourse and had used tampons, whereas it was easily inserted in 81% of sexually active patients. The same study revealed that subjects who were not sexually active had comparable gynecologic and hymenal findings regardless of tampon (versus pad) use, sports activities, or prior pelvic examination. Nonetheless, hymenal rupture in the absence of sexual activity has been associated with prior surgery, tampon insertion, physical exercise, and masturbation.48–50 Conversely, intact, nondisrupted hymens were reported in 52% of women who had prior sexual intercourse.51 Bleeding may not occur, or the repair of sufficient strength may necessitate hymenotomy or surgical transection.52 For Muslim patients, physicians should make the distinction that although premarital or extramarital sexual relationships are strictly prohibited, proof of virginity by bleeding on the wedding night is not necessary.19 All women (and family members) who present for restoration of the hymen with the intent to elicit postcoital bleeding as a sign of virginity, should be informed that no specific genital findings distinguish prior sexual abuse from non-abuse-related conditions.44 In most reviews, the surgical technique is vaguely described, and success rates are either not reported or reported as low, with a 67% success rate in one study.53 However, surgical approaches can be categorized as surgical flaps, surgical adhesions, lumenal reductions, suture-only techniques, or artificial membranes/reservoirs. The timing between the procedure and coitus is a critical issue that generally receives little attention. One author discussed practitioners even performing the procedure “in the days immediately before the wedding.”54 I have learned much about it from personal communication with other practitioners. For patients who desire structural integrity and need the hymen to be intact on visual inspection, the repair should be performed 3 months before the “consummation of marital vows.” However, when the timing of coitus is known, and the patient desires bleeding but visual integrity is not needed, surgery is often best scheduled 3 weeks before the date. In patients with partial wound breakdown, granulation tissue is sufficient to promote bleeding with the lightest of friction. van Moorst et al1 suggested performing surgery no sooner than 14 days before the wedding to increase the chance of blood loss, but not much later to prevent visibility of the suture remnants. Nearly all patients have marked anxiety because of the preceding events or because they are sexually introverted; thus I advise them to have general anesthesia or monitored anesthesia care with appropriate perioperative medications. Local anesthesia with or without oral or intravenous sedation, or monitored anesthesia care, is occasionally performed for patients extremely at ease, such as those celebrating a second honeymoon, those willing to tolerate the injections, and those with time for repair. In these cases, a Telfa pad rolled into a tampon is inserted into the distal vagina. The tampon is removed immediately after the patient is positioned but before the injection and prep. The purpose of the Telfa pad is to apply pressure and direct apposition of the topical cream to the circumferential hymenal fragments rather than allow gravitational settling along the posterior wall. No controlled studies call for the use of antibiotics, but they are given in accordance with reports showing their benefits in third-degree postpartum perineal wounds.55,56 Patients are placed in a lithotomy position and prepped in a routine sterile fashion. Very limited discussions of the vaginal mucosal flap procedure are available and only briefly mentioned as a second option when hymenal remnants are insufficient. The description of the entire procedure is simply, “… a narrow strip of posterior vaginal wall is dissected for reconstruction.”14,30,57 It is rarely, if ever, performed, because it requires a repair that is sufficient to remain intact yet weak enough to rupture with penile penetration. If true squamous epithelium healing occurs, the flap may necessitate surgical release. The most popular technique by far involves surgical adhesions.57,58 However, one of the most commonly described articles cited only nine cases performed over 10 years.46 The author based his technique on a publication mentioned in a previous publication (with 20 cases and no follow-up physical examination).30 The surgical method was briefly mentioned in 29 words. I have described my surgical adhesion technique in detail later in the chapter. In an overview of female genital plastic surgery, Goodman59 discussed two techniques. He reported on one method of circumferential decrease in caliber of the introitus using multiple, small, diamond-shaped excisions along the periphery of the hymenal ring and the more common method of denuding opposing hymenal fragments followed by surgical adhesion. Although the Goodman technique achieves a luminal reduction with multiple side-to-side approximations of hymenal fragments using diamond-shaped excisions between the remnants, the surgical adhesion technique results in luminal obstructions through end-to-end approximation of hymenal fragments (Fig. 12-2).
Hymenoplasty
Otto J. Placik
Key Points
General Considerations
Ethical and Cultural Considerations
Elective Versus Reconstructive Surgery
Indications and Contraindications

Patient Evaluation
Clinical Evaluation of the Deformity
Preoperative Planning and Preparation
Surgical Techniques
Anesthesia, Antibiotics, and Markings
Patient Positioning
Flap Technique
Surgical Adhesions
Lumenal Reductions
Related posts:
 Fractional Erbium Laser for Vaginal Rejuvenation
Fractional Erbium Laser for Vaginal Rejuvenation
 Labia Majora Reduction Surgery: Majoraplasty
Labia Majora Reduction Surgery: Majoraplasty
 Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
Anatomy and Classification of the Female Genitalia: Implications for Surgical Management
 Psychological Issues and Social Mores in Female Genital Aesthetic Surgery: What Is Normal?
Psychological Issues and Social Mores in Female Genital Aesthetic Surgery: What Is Normal?
 Augmentation of the Labia Majora With Fat Grafting
Augmentation of the Labia Majora With Fat Grafting
 Perineoplasty and Vaginoplasty
Perineoplasty and Vaginoplasty
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine
