Anatomically Placed Bone Tunnels
Anatomically placed bone tunnels are usually easily revised, as in most cases they are simply reused after hardware removal. However, tunnel widening may be a problem and should be addressed by utilizing bone plugs, careful choice of graft material, stacking of screws (Fig. 10.1), or prior bone grafting.

Fig. 10.1
Radiograph of stacked screws in the tibia bone tunnel in mildly expanded bone tunnel. Reprinted from ref. [3] with permission from Elsevier
Non-anatomically Placed Bone Tunnels
Malpositioned Bone Tunnels That Do Not Interfere
Non-anatomic bone tunnels that do not interfere with the new revision bone tunnels can be left alone, and the primary fixation devices are removed only when necessary. Major malposition of the tibial tunnel is most often too posterior with a femoral tunnel high in the notch, the so-called vertical graft. In case of too anterior location of the tibia bone tunnel, there is risk of notch impingement and loss of full extension. In both cases, it is fairly easy to perform a revision ACL reconstruction as the material and bone tunnels are usually severely malpositioned and do not interfere with the new anatomically placed bone tunnels (Figs. 10.2, 10.3, and 10.4). This “divergent tunnel” concept allows the surgeon to address severely malpositioned bone tunnels and avoid preexisting hardware that is often difficult—and unnecessary—to remove.


Fig. 10.2
Too anteriorly placed previous bone tunnel that does not interfere with the new anatomically placed tibial bone tunnel
Fig. 10.3
Malpositioned too anterior tibial bone tunnel and “high” femoral bone tunnel
Malpositioned Bone Tunnels That Interfere
Difficulties arise when the non-anatomic bone tunnels overlap with the new revision tunnels. This often presents a major challenge as it can cause potential complications such as inferior fixation strength and fracture. Several methods can be used to cope with this difficulty.
Divergence of the new and old bone tunnels is essential. However, the intra-articular entry point should always attempt to exit at the native footprint of the ACL. This can result in convergence and a “figure-eight” defect (Fig. 10.5) [3]. In these cases, the small bone bridge between the bone tunnels is often inadequate for secure fixation and there is little good-quality bone to allow graft-bone healing. There are several available methods to address this dilemma:
Fig. 10.5
The so-called figure-eight after anatomic ACL revision reconstruction with a prior malpositioned tunnel. Reprinted from ref. [4] with permission from AAOS
Bone grafting with large autologous bone plugs and/or bone chips from the iliac crest.
Utilization of bioactive implant material such as moldable calcium phosphate cement [5].
Utilization of an ACL tendon graft with a large bone plug such as an autograft quadriceps tendon or allograft Achilles tendon.
Utilization of extra-cortical fixation instead of aperture fixation in order to avoid stress on the small bone bridge between the bone tunnels.
Divergent extra-articular tunnel orientation as the tibial footprint can be approached from multiple angles by using different starting points, even from the lateral side of the tibia (Fig. 10.6) [6].
Fig. 10.6
Lateral tibial tunnel can be utilized in severe cases where there are difficulties creating a divergent bone tunnel due to tunnel widening and near anatomical position. Reprinted from ref. [6] with permission from WB/Saunders Co.
Tunnel Widening
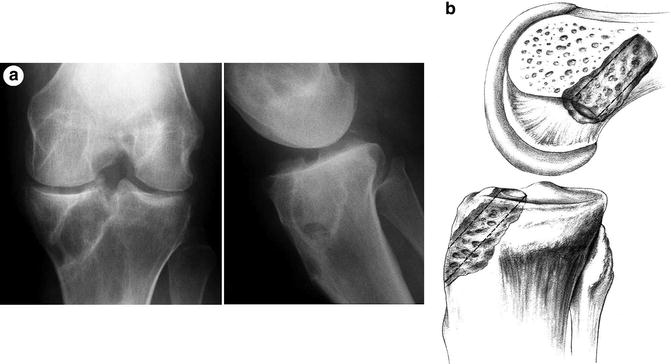
Surgical options for a one-stage revision are more limited when the tibial bone tunnel exceeds 15 mm or is very close to the planned new tunnel (Fig. 10.7). The main reason is that the tunnel widening will compromise secure fixation. Bone grafting can be performed in a two-stage procedure if necessary.
Get Clinical Tree app for offline access
Fig. 10.7
Radiograph (a) and illustration (b) depicting a large tibial defect and tunnel widening. Figure (a) reprinted from ref. [3] with permission from Elsevier; Figure (b
 Graft Selection for Revision ACL Reconstruction
Graft Selection for Revision ACL Reconstruction
 Indications for Revision ACL Reconstruction
Indications for Revision ACL Reconstruction
 Technical Causes of ACL Graft Failure
Technical Causes of ACL Graft Failure
 Single Stage ACL Revision Reconstruction: Indications and Technique
Single Stage ACL Revision Reconstruction: Indications and Technique
 Avoiding the Failed ACL: How to Prevent ACL Tears Before They Occur
Avoiding the Failed ACL: How to Prevent ACL Tears Before They Occur
 Fixation in Revision ACL Reconstruction
Fixation in Revision ACL Reconstruction




Related posts:
Graft Selection for Revision ACL Reconstruction
Indications for Revision ACL Reconstruction
Technical Causes of ACL Graft Failure
Single Stage ACL Revision Reconstruction: Indications and Technique
Avoiding the Failed ACL: How to Prevent ACL Tears Before They Occur
Fixation in Revision ACL Reconstruction
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
