Fig. 9.1
Tunnel widening

Fig. 9.2
Bone graft as cylinder
4.
It is impossible to remove prior hardware or create a new tunnel.
This is an uncommon situation and one should consider an over-the-top procedure if this is encountered. The graft can be taken over the top of the lateral femoral condyle and fixed through a lateral incision. Alternatively, the divergent tunnel concept can be useful in this situation if it is possible to bypass the hardware and recreate the anatomical ACL femoral footprint.
5.
Revision after failed double-bundle reconstruction.
(a)
Both tunnels are in the wrong position and cannot be reused.
If both the tunnels are completely incorrect and cannot be reused, then a two-stage procedure is considered because of the high risk of fracture. In the first stage, bone grafting is done by impaction of a cylindrical iliac crest autograft or allograft. If CT scan at 3–6 months shows a good bony fill, the second stage of the procedure of revision ACLR can be performed.
(b)
One of the tunnels (Anteromedial or Posterolateral) can be reutilized.
Leaving the reusable tunnel, the other new tunnel is created after removing the hardware (if necessary) and a single-bundle ACLR is performed, as indicated.
(c)
The two tunnels are too close or there is a breakage of the wall between them.
In such a situation we would consider a single-bundle revision, a two-stage procedure, and/or a suspensory fixation, as indicated.
Finally, preoperative patient education is extremely important prior to a revision procedure and the expectations of the patient should be modified. Revision ACL surgery represents a salvage procedure and the patient should be counseled that the outcome is not likely to be as good as a primary procedure. The goal of surgery is to provide a stable pain-free knee. Return to sport is another goal, but is less predictable. In many cases, the status of the articular cartilage and meniscus are major factors in determining return to sport.
Over-the-Top Technique
Femoral tunnel creation is a key to revision surgery. In some cases, due to compromised bone, it can be very difficult to create a new femoral socket. In addition, the effectiveness of femoral bone grafting has not been well elucidated in the literature [5]. In cases with severe tunnel widening on the femoral side, it may be impossible to create a new tunnel in a single-stage procedure. In such situations, we recommend considering the over-the-top of the lateral condyle procedure for femoral fixation [6].
Case Example of Over-the-Top Femoral Fixation in Massive Bone Loss
The patient was a 42-year-old competitive Judo player who presented with reinjury after single-bundle ACL reconstruction with semitendinosus autograft at 11 years previously. Computed tomography revealed massive bone resorption around the original femoral insertion site (Fig. 9.3a, dotted line). Revision surgery was planned using a BTB graft. Arthroscopic inspection after debridement of soft tissue revealed that the bony surface area behind the enlarged femoral tunnel aperture was insufficient for creating a new tunnel without overlapping (Fig. 9.3b, c). We therefore switched to go over-the-top of the lateral condyle via the posterior capsule for fixing the graft to the femur (Fig. 9.3d, e). On the tibia, we created a new tibial tunnel from the tibial cortex more medial than the previous one to the same aperture, as it was properly located in the center of the anatomical attachment site. Thus the wall of the new tunnel was mostly composed of fresh cancellous bone, as shown by intra-tunnel arthroscopic observation (Fig. 9.3f). The patient was able to be back to strenuous activity by 8 months post-surgery without any complaints of knee instability.
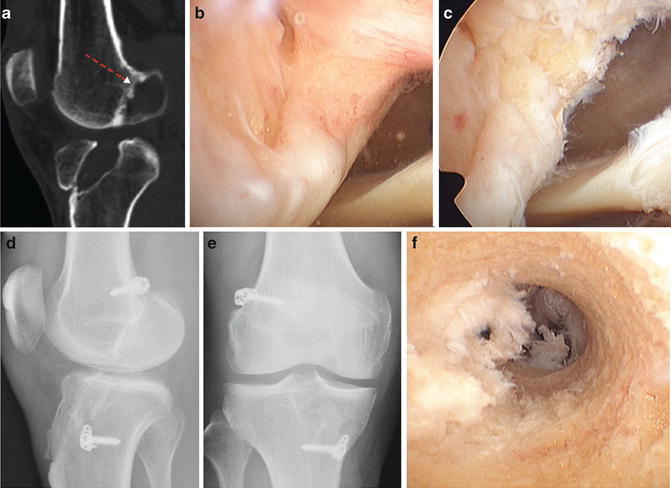
Fig. 9.3
An illustrative case with bone absorption. (a) CT of the right knee before revision. Note the severe bone absorption around the anatomic femoral attachment (dotted line); (b, c) postoperative lateral (b) and AP (c) radiograph showing femoral graft fixation over top of the lateral condyle; (d) arthroscopic view of femoral tunnel aperture from anterior medial portal; (e) after debridement, posterior wall consists of fatty tissue without bony structure; (f) intra-tunnel view of the newly created tibial tunnel. Note most of the wall surface is composed of cancellous bone
Anatomic Rectangular Tunnel (ART) Technique
We developed the anatomic rectangular tunnel ACL reconstruction (ART ACLR) with a BTB graft to mimic natural fiber arrangement inside the native ACL and to minimize tunnel size aiming at reducing the space between the graft and tunnel walls [7–9]. The ACL femoral attachment area is of crescent shape, less than 10 mm in width, and located at the superior–posterior margin of the lateral wall of the notch, as shown in published studies [10–14]. The technique makes it possible to create the tunnel aperture inside the attachment area. A tunnel aperture within the thicker cortical area of the femoral attachment area may be more robust, and may potentially reduce the tunnel widening [15].
When planning to use a 10-mm wide BTB graft for revision, the procedure is advantageous not only to avoid overlapping tunnels in case of improperly placed tunnels from the previous surgery but also to leave more space between the old and new tunnels. The cross-sectional area of the tunnels of 50 mm2 (5 × 10 mm) in ART ACLR is less than that in a conventional 10-mm round tunnel technique of 79 mm2. Since tunnel encroachment would hypothetically be less of a problem, we presume the ART ACLR technique could be more easily applied as a one-stage revision procedure after failed primary ACLR.
Surgical Principles for Anatomic Rectangular Tunnel Technique
The principles are to (1) create parallelepiped tunnels with rectangular apertures inside the anatomic attachment areas (Fig. 9.4), (2) avoid overlapping tunnels or staged operations (Fig. 9.5), and (3) accept the preexisting tunnel apertures if they were in the anatomic attachment areas.
Fig. 9.4
Intra-articular tunnel apertures of the femur (a) and the tibia (b) in anatomical rectangular tunnel ACL reconstruction (ART ACLR). (a) Note the tendinous side of the bone plug (black-painted area) located posteriorly superiorly in the femoral tunnel; (b) the tibial tunnel is almost filled with the tendon (black-painted area)
Fig. 9.5
Schema of revision rectangular tunnel ACL reconstruction with (BTB) graft. The bone plug is fixed to the femur with a 6-mm IFS, whereas tibial fixation is achieved with a modified pullout suture technique using the DSP (Double Spike Plate) and a screw. With this procedure, the new anatomical femoral tunnel can be properly placed in most cases without overlapping tunnels despite the previous high and anterior femoral tunnel (PHFT) leading to a vertical graft. In most cases, a new tibial tunnel is created with the same aperture as the previous vertical tibial tunnel (PVTT), whereas the direction is changed
The patient is positioned supine with the thigh in a leg holder. The anteromedial portal is used for viewing and the far anteromedial portal for instruments [16]. The femoral tunnel is created using an all-inside technique through the far anteromedial portal with the knee flexed beyond 140°. If the knee cannot be flexed beyond 140°, this step can also be accomplished in outside-in fashion via a small lateral thigh incision. The tibial tunnel is created through the anteromedial cortex to the anatomic intra-articular insertion. Two continuous 5-mm tunnels along the long axis of the attachments are created and then dilated with a 5 × 10 mm dilator into parallelepiped tunnels [8




Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
