4 High Brow Approach to Neuromodulators
Summary
Although women represent the majority of patients seen in many aesthetic practices, the number of male patients is increasing. This heightened demand has been attributed to a multitude of factors including interest in enhancing one’s appearance, ageism, competition in the workplace, increasing acceptance of cosmetic procedures, as well as ever-growing societal and social media pressures. Botulinum toxin A (BTX-A) treatments constitute the most popular minimally invasive cosmetic procedure by far. Whereas the general principles of BTX-A treatment for men and women are similar, it is important to acknowledge unique male characteristics that impact assessment and treatment paradigms. Attending to the distinctive needs of the male patient is paramount in order to achieve optimal clinical outcomes and enhance the overall patient experience.
Keywords: botulinum toxin botulinum neurotoxin A botulinum toxin serotype A neurotoxins neuromodulators BTX-A male men
4.1 Background
The introduction of botulinum toxin A (BTX-A) to the armamentarium of cosmetic practitioners has revolutionized the field of facial rejuvenation, initiating a seismic shift in patient preferences in favor of minimally invasive procedures. In the past 15 years, BTX-A injections have become increasingly popular as a noninvasive cosmetic procedure with a 759% increase.1 Whereas women much more commonly undergo BTX-A treatments, the number of men availing BTX-A injections has increased by 337% since 2000.2 Men are becoming increasingly attentive to their appearance, and societal norms are evolving to create a more accepting environment for men to express their concerns and seek appropriate treatments. According to the American Society for Aesthetic Plastic Surgery, 1,638,940 women and 162,093 men underwent BTX-A treatment in 2018. Men constituted 9% of BTX-A treatments and this number continues to increase.3 According to the American Society of Plastic Surgeons, botulinum toxin treatments were by far the most popular minimally invasive procedure in males in 2018 with a 41% share, an almost threefold margin over laser hair removal, the second-most popular.4
4.1.1 Motivation
From 2000 to 2018, the use of BTX-A among men increased by 381% according to the Plastic Surgery Statistics Report conducted annually by the American Society of Plastic Surgeons.4 Even though BTX-A reduces unwanted wrinkles and rejuvenates the skin, vanity is not the only motivator behind decisions to undergo such treatment. This increase in the rate of BTX-A injections among men may be attributed to multiple factors. First and foremost, from an evolutionary perspective, an improved appearance is always desirable.5 BTX-A treats wrinkles, thus softening facial lines, improving skin quality, and enhancing the overall appearance of the face.6 Second, given that ageism exists in some workplaces, an aged appearance could potentially interfere with promotions, career opportunities, and personal growth.7 As a result, men have shown more interest in receiving BTX-A injections to improve their appearance and become more competitive with their younger-looking colleagues. Third, there are shifting expectations around aging. As life expectancies rise, so are expectations for graceful aging. According to a project led by Dr Scherbov, from the International Institute for Applied Systems Analysis in Austria, given that life expectancy is increasing, people are now being viewed as “old” when they hit 65.8 Men who are in their 60 s do not feel their age and thus avail themselves of noninvasive procedures such as BTX-A injections to maintain a youthful appearance that better matches how they feel. Finally, social media has become an integral part of society that has generated enormous pressures to look youthful. According to a report conducted by Nuffield Council on Bioethics, pressure from social media is linked to a significant rise in cosmetic procedures such as BTX-A injections.9
4.1.2 Demographics
Data on the demographics of men undergoing BTX-A injections are limited. According to the 2018 Plastic Surgery Statistics Report,4 1% of men undergoing BTX-A treatment fell into the age range between 20 and 29 years, followed by 18% of those who were in the age range between 30 and 39 years, 57% were in the age range between 40 and 45 years, whereas 23% were aged 55 and over.
In a recent systematic review by Roman and Zampella on 19 randomized controlled trials (RCTs) on BTX-A injections for facial rhytids and 22 RCTs on hyaluronic acid injectable fillers for soft-tissue augmentation, men represented 11.8% of all patients and 13.9% patients receiving BTX-A.10 Caucasian patients represented 67.1% of the total patients, whereas Asian, Hispanic, and black patients represented 16.8, 6.5, and 5.4% of study participants, respectively.
4.2 Anatomy
4.2.1 Assessment of the Face
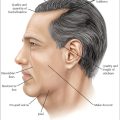
When assessing the male face (Fig. 4.1), care must be taken to review not only the musculature that is to be targeted with neurotoxin (Fig. 4.2) but also the skeletal shape, vasculature, and the hairline. This ensures that the physician takes into account sexual dimorphism, which is the intraspecies phenotypic difference between sexes.11
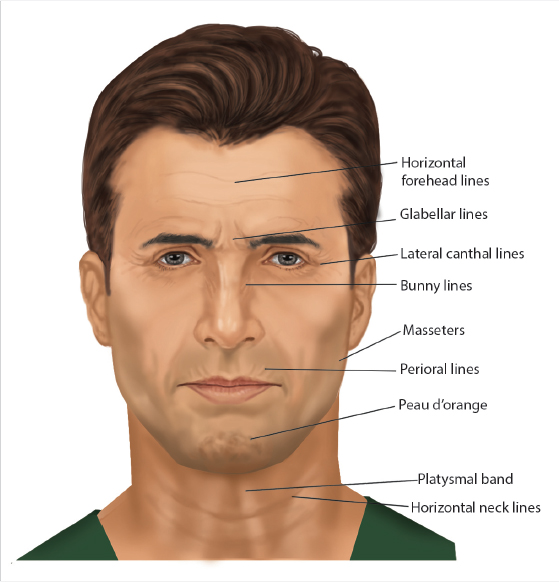
Fig. 4.1 Facial areas amenable to neuromodulator treatment.
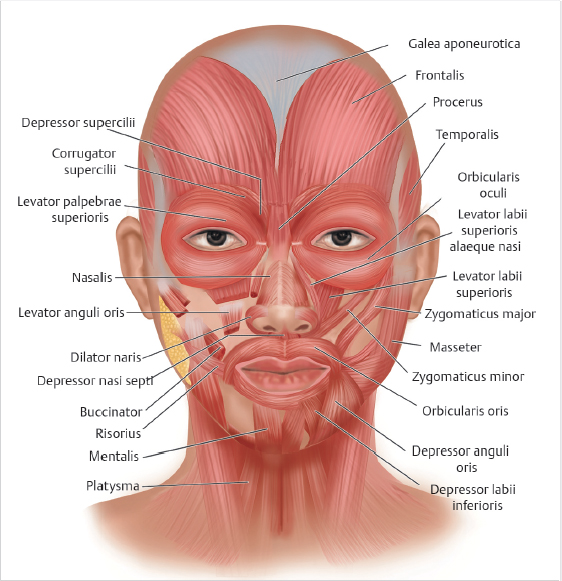
Fig. 4.2 Facial muscles relevant to botulinum toxin treatment. Note the close muscle interrelationships.
Bone
There are a number of differences between the male and female skull (Fig. 4.3). Men are characteristically seen to have larger skulls than females. In reality, this reflects the observation that female skulls are roughly 80% the size of male skulls.12,13 Starting at the more anterior aspects of the skull, men appear to have a higher, wider, flatter, and greater sloped forehead compared to females.11,14
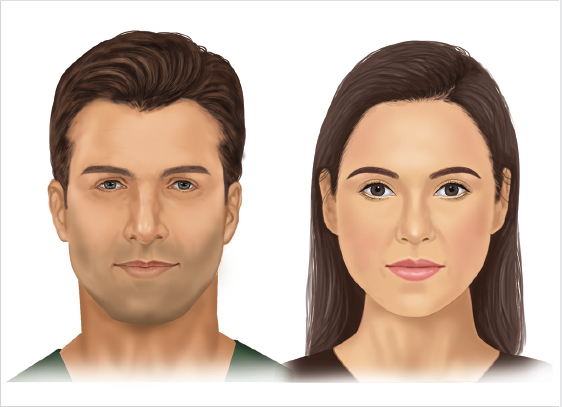
Fig. 4.3 Youthful male and female faces. Detailed knowledge of gender differences is important in optimizing male aesthetic treatment outcomes.
Looking at the periorbital area of the male skull, the supraorbital ridge is more prominent in males, giving greater glabellar anterior projection and acting as the common landmark for male brow position.11,12,15,16 In contrast, the female supraorbital ridge is less prominent, with the brow positioned just superior to the ridge.17 The shape of the male brow is often flat, whereas the female brow usually peaks or arches in its lateral third portion.17,18 Additionally, the male orbits themselves frequently have a larger height and a less oval shape.19
The more notable skeletal differences on the lower portion of the face between sexes are in the cheeks and chin.12,20,21 Male cheeks or zygomas are frequently flatter but more angulated than females.20 Finally, the male chin is seen as wider and larger than females, with male chins also having more anterior projection.21
Musculature
Males have approximately 1.5 times more muscle mass overall than females, yet studies are lacking that confirm if this increase also specifically applies to facial muscle mass.22 After adjusting for facial size, men also appear to have greater facial muscle movement during lip pursing, cheek puffing, and eye-opening animations.23 A 2009 study showed that males have greater upward motion in both of the study’s analyzed facial movements—posed smile and lip pucker.24 With regard to rhytid formation, a 2013 Japanese study of 173 males and females aged 21 to 75 years found that men have greater forehead rhytid formation across all age groups.25 Furthermore, the study found that males had statistically significant higher rhytid scores in additional facial areas within specific age categories: 21- to 28-year-old males had higher glabellar, nasal root, and cheek rhytid scores; 35- to 41-year-old males had higher nasal root rhytid scores; and finally 47- to 59-year-old males had higher periocular rhytid scores.25
Males do not have more rhytids in all facial areas. For example, aging females typically have deeper rhytids than males in the perioral area.25,26 This may be due to smaller size of the perioral pilosebaceous unit in females compared to males.26 Thicker adipose layers are seen in female faces, which could also explain why females often have fewer or more shallow rhytids than in their male counterparts.11,27 Of note, it has also been shown that male skin, including facial skin, can be 10 to 20% thicker than in women, which may impact injection technique.28
Certain facial rhytid patterns are more commonly seen in men secondary to larger facial muscle bulk and recruitment of nearby muscles.12 For example, the “U” glabellar wrinkle pattern is seen more often in men as a result of their larger procerus muscle.29 Men also more commonly have a downward fan lateral canthal wrinkle pattern, whereas women are seen to have central, full, or downward fan patterns.30 The higher prevalence of the downward fan pattern in males may be secondary to greater recruitment of the zygomaticus major muscle.12
Some authors also suggest that the corrugator supercilii are broader in men and their distal fibers extend more laterally than in females.31 The same author emphasizes that the frontalis is more sheetlike in men, whereas in women, it is thought of as two separate muscle bellies with absent or reduced central muscle mass.31 Both of the aforementioned differences should be considered when planning injection patterns in male patients.
Vasculature
There appears to be an increase in vasculature in the male face when compared to the female face.32,33 It has been hypothesized that this finding is secondary to the increased blood supply needed for the coarse terminal facial hairs in men.11 Furthermore, an increase in the number of dermal capillaries often corresponds to greater diameter of the patient’s hair follicles.34 This increase in local vasculature is thought to increase a male’s bruising risk with facial neurotoxin injection.11 However, given that the increase in vasculature is thought to be located in areas of coarse facial hair, Keaney and Alster postulate that injecting the frontalis would not carry a similar increased risk of bruising.11
Hairline
A regression of the anterior, especially the anterolateral, aspects of the hairline can often occur in male androgenic alopecia.12,35 As a result of this regression, the male forehead can appear larger.12 The authors suggest that care should be taken to assess the most superolateral aspects of male forehead rhytids, especially if the patient has androgenetic alopecia, as failure to treat this area could draw unnecessary attention to a receding hairline.
4.3 Approach
Male patients have varying degrees of knowledge about BTX-A treatments, making it important to take the time to fully explain the process, and set realistic expectations to optimize patient satisfaction.12 Male patients are also more likely to seek out cosmetic procedures that require less downtime and fewer visits.12,36 The authors suggest booking a follow-up visit for all newly treated patients 2 to 3 weeks after treatment in order to optimize outcomes, build trust, and improve retention rates. Data suggest that male patients are less likely to return on their own even if they deem the outcome less than desirable.12,37
Minimal data exist that specifically address male neurotoxin dosing with most of it focusing on the glabella. Given increased muscle mass and strength, men generally tend to require higher doses than women.38 As with all medical procedures, neurotoxin treatments must be individualized based on unique male characteristics in order to achieve optimal clinical outcomes and enhance the overall patient experience.
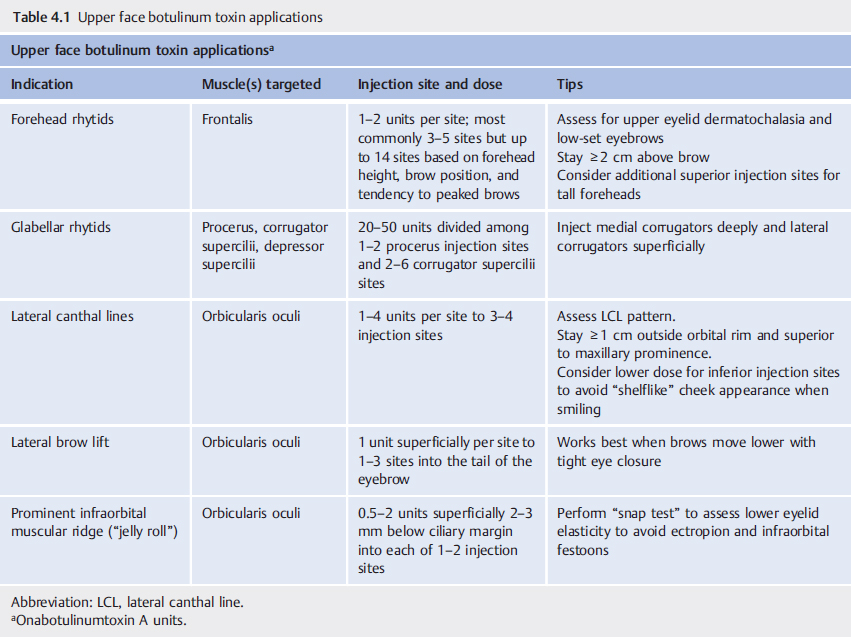
The approach to BTX-A treatment involves proper assessment of muscle bulk and activity with corresponding vectors of movement (Fig. 4.4), as these determine dose required and treatment pattern, respectively.70 For the purposes of this chapter, dosing will be stated in onabotulinumtoxinA equivalents unless otherwise noted and the focus will primarily be on treatment of the upper face (Table 4.1). It is important to note that dosing between BTX-A formulations is not interchangeable and units cannot be converted on a 1:1 basis.
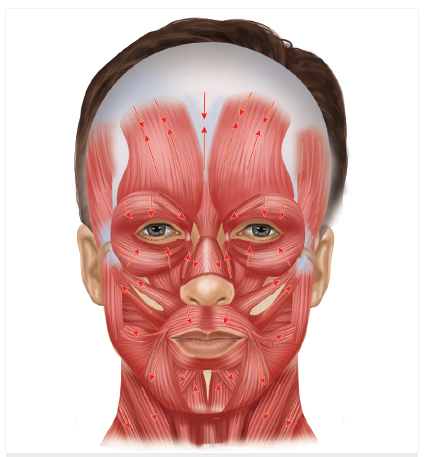
Fig. 4.4 Facial muscle vectors. Understanding precise muscle activity allows one to customize treatments and optimize outcomes.
4.3.1 Forehead and Brow
Brow height, shape, and position are key determinants of nonverbal cues perceived by others and overall facial appearance. Brow ptosis occurs naturally over time, making careful inspection of brow height critical when assessing the upper face.12,39 Although the product monograph recommends injecting at least 2 cm superior to the eyebrow to reduce the risk of neurotoxin-induced ptosis, the authors suggest considering individual anatomy and muscle depth so as to avoid lowering the brow by inadvertently targeting the frontalis muscle.35,40 Males typically have more noticeable forehead rhytids as they may contract the frontalis more frequently in order to raise the brow and maximize visual fields.31 Many males have a tall forehead, meaning that one row of injections may not be adequate to achieve the desired degree of wrinkle reduction. Thus, in some cases, two rows of four to eight injection points may be needed to fully treat upper and lower frontalis rhytids.12,39,41 One author suggests approaching this in two visits, treating the upper forehead lines at the first visit, and then subsequently treating any residual lower forehead lines at a second appointment.31 It is also important to assess the most superolateral aspects of the forehead in male patients with a receding hairline to determine whether or not additional neurotoxin injections in this area would help reduce wrinkles in the area of temporal recession.20,37,39,41 The authors recommend starting with conservative forehead dosing given that the frontalis is highly responsive to treatment. Additionally, because the frontalis muscle is the only brow elevator, it should not be injected without also treating the glabella. Failure to do so will result in unopposed brow depressor activity and could theoretically contribute to medial brow ptosis, especially in older male patients.
The line of convergence (C-line) is a more recently introduced concept42 that describes a horizontal line located at approximately 60% of the total forehead height measured from the orbital rim. Below this line, the frontalis muscle lifts the eyebrows, while above the C-line, it depresses the hairline. It is important to consider this during forehead injection planning.
Given that most men prefer flatter brow shape, it is important to consider lower lateral frontalis activity when treating the forehead. In men with prominent activity in this area, failure to treat may lead to overly peaked lateral brows, resulting in a more feminine brow appearance.12,31,37,39,41 To avoid this, or to rectify it if it occurs, 2 units of onaBTX-A/incoBTX-A or 6 units of aboBTX-A may be injected into the lower lateral frontalis above the lateral brow or where the brow is peaking.12,31,41 Caution is advised in individuals with upper eyelid dermatochalasis.
In less common instances where a browlift is desired in men, two approaches are suggested by one author. Treatment of only the medial aspect of the glabella, the procerus muscle, can result in elevation of the medial brow,31 whereas neurotoxin injection into the most lateral aspect of the eyebrow targeting a portion of the orbicularis oculi muscle will elevate the lateral brow.31 Both techniques can be combined if complete brow elevation is desired.31 A 2016 paper by Scherer recommends a different approach for a browlift in men, which aims to raise the entire brow without a change in shape.39 This author utilizes four injection points along the length of the superior aspect of the eyebrow itself to relax the corrugator and the upper orbital portion of the orbicularis muscle.39 Moving medial to lateral, the injection points include the head of the eyebrow, followed by an intermediate point, then a third injection in the relative brow curvature point, and finally into the brow tail.39 That author suggests 2.5 to 5 units per injection point, except for the medial head of the brow where 5 units are recommended.39
A large consensus developed recommendations in 2017 for incoBTX-A injections into male and female foreheads.38 They divided the forehead into 12 zones (3 vertical by 4 horizontal) with the lowest four zones positioned 1.5 to 2 cm superior to the eyebrow to lower the risk of brow ptosis.38 Separate protocols were developed for males and females, each being subdivided into normal kinetic, hyperkinetic, and hypertonic.38 Other considerations impacting their recommended doses included forehead size, presence of palpebral weakness, hairline, and tendency to develop a Mephisto sign (“Spocking” or peaked brow).38 The dose per injection point did not exceed 1 unit in hypertonic males or females. Slightly higher varying doses of 1 to 2 units per injection point are recommended in hyperkinetic males and females.38 Similarly, the suggested doses for normal kinetic males and females per injection point are 1 to 2 units.38 However, one exception is a recommendation of 3 units into each of the two central forehead zones if the normal kinetic male has palpebral weakness.38
4.3.2 Glabella
The glabellar complex consists of left and right corrugator supercilii muscles and the central procerus muscle that pull the brows inferomedially with contraction. When treating the glabellar area, patients should be examined both at rest and at maximal frown. The authors find it helpful to rate glabellar frown severity as mild, moderate, or severe based on the depth and width of the wrinkles. This, combined with muscle bulk, helps guide BTX-A dosing, with higher dosing required in cases of more severe dynamic wrinkles and larger muscle bulk. It is imperative to keep in mind that deep static glabellar lines, colloquially referred to as “the 11 s,” are not commonly eliminated with neurotoxin treatment alone and that complementary soft-tissue filler treatment may be required to improve the contour and smoothen the “hill and valley” glabellar appearance that is sometimes evident. Interestingly, the authors find that repeated, consistent BTX-A treatments do sometimes eventually significantly improve static wrinkles.
The muscles of the glabellar complex interdigitate and are intimately related. Because of this, knowledge of anatomy and muscle depth is critical in order to maximize efficacy and minimize complications that may arise by inadvertently treating adjacent muscles. Asking the patient to frown allows the belly of the procerus and corrugators to be visualized and grasped between the thumb and the index finger, facilitating injection accuracy. Whereas Food and Drug Administration (FDA) product monographs for all approved BTX-A products suggest staying at least 1 cm above the bony supraorbital rim when injecting the corrugators, the authors recommend individual evaluation in order to allow treatments to be tailored to the individual’s unique anatomy. Note that injecting the glabellar area could potentially stimulate the trigeminal nerve and thus trigger a sneezing sensation or response.
The first injection is centrally placed perpendicularly into the procerus over the area of greatest muscle bulk. If the procerus muscle is long and demonstrates significant activity, two separate midline injection sites rather than the standard single injection may be advantageous.43 Once again, injection depth must be tailored to procerus muscle depth with more inferior injections being deeper than more superior ones. Given that more men appear to have a “U” glabellar pattern, injecting both the superior and inferior portions of the procerus muscle may be advisable.29
When injecting the corrugators, it is important to consider the origin and insertion of the muscle. Because the corrugator originates on bone medially and then becomes more superficial laterally, interdigitating with the frontalis muscle, it is best to inject deeply medially and more superficially laterally. Failure to inject superficially laterally may result in brow ptosis due to inadvertent weakening of the frontalis muscle. The number of injections will be determined by factors such as the extent of the corrugator muscle and the desire to avoid brow ptosis in individuals with low-set brows, as detailed later.
Glabellar BTX-A injection patterns are best determined based on the five described muscle contraction patterns, namely, the “U,” “V,” “omega,” “converging arrows,” and “inverted omega” dynamic wrinkle patterns.44 In Koreans, the patterns described include “U,” “11,” “X,” “π (pi),” and “I.”29
Care should be taken to assess brow position, shape, and symmetry when treating the glabellar complex. All of this must be done in conjunction with assessment of the forehead as the frontalis muscle greatly influences brow position, serving as the only brow elevator. If the brows are asymmetric, it is important to point this out to the patient prior to treatment. In deciding how to proceed in such cases, analysis of the medial, central, and lateral portions of the brow should be considered. When the medial portion of the brow is low, this may sometimes be corrected by injecting the belly of the medial corrugator muscle deeply over the inferomedial portion of the brow, thus reducing the downward pull of the medial head of the corrugator muscle, thus allowing for more superolateral positioning of the medial brow. On the other hand, if the lateral portion of the brow is low, this may be due to contraction of the descending lateral orbicularis oculi muscle fibers that pull the tail of the brow inferomedially in a purse-string fashion. Ascertaining the contribution of lateral orbicularis oculi activity to lateral brow position may be done by asking the patient to tightly close the eyes and observing changes in brow position. When the lateral brow moves inferomedially, this implies that the orbicularis oculi muscle plays a significant role in lowering the lateral brow and, thus, a series of one to three low-dose BTX-A injections into the tail of the brow can minimize the downward pull and lead to lateral brow lift. Conversely, if there is no downward movement of the lateral brow when tightly closing the eyes, such injections are unlikely to help lift the lateral brow.
Brow position and eyelids must be assessed carefully prior to treating the glabellar complex. Individuals who manifest upper eyelid dermatochalasis or who have naturally low-set brows may be at higher risk of brow ptosis with treatment of the glabella. Injection of the lateral corrugators may weaken the lower frontalis fibers, causing the brows to drop and eyelids to become heavier. Thus, in these cases, it is critical to reduce the number of lateral injection sites and/or dose of BTX-A. Alternatively, lateral corrugator treatment may be omitted altogether as an added precautionary measure. Unfortunately, this will lead to residual lateral corrugator activity, leading to medial movement of the skin and thus contributing to incomplete effacement of glabellar furrows. Patients that desire a more “frozen” look over the glabella must be advised that this may come at the expense of heavier brows and eyelids, potentially producing a more tired appearance.
One of the first neurotoxin dose response studies in men was published by Carruthers and Carruthers in 2005.45 The study evaluated 20-, 40-, 60-, and 80-unit doses of BTX-A distributed among seven glabellar complex sites in 80 men.45 The 40-, 60-, and 80-unit doses were consistently more effective with longer duration, higher peak response rate, and greater improvement from baseline compared to the 20-unit dose in a dose-dependent manner. Importantly, the incidence of adverse events was not increased with higher doses.45 The authors concluded that the FDA- and Health Canada–approved glabellar dose of 20 units of BTX-A is too low in male patients and they recommended starting at 40 units.
A randomized, placebo-controlled study of 50 units of aboBTX-A for glabellar lines found that women had a substantially better response as measured by none or mild wrinkles at day 30 than men (93 vs. 67%).46 The authors similarly concluded that 50 units of aboBTX-A is too low of a starting dose for the male glabellar complex.46
A second randomized, placebo-controlled trial of aboBTX-A injection into the glabellar complex was conducted with dosing adjustments based on gender and glabellar muscle mass.47 Male patients enrolled in the study received 60 to 80 units of aboBTX-A, whereas female dosing ranged from 50 to 60 units. Overall, despite higher dosing, males were still less likely to respond than females; however, the response rate was higher than that reported by other studies using 50 units of aboBTX-A.47
A 2009 study suggested a 7-point injection approach for treating the glabella where all injections are located between the midpupillary vertical lines and focus on targeting the lateral corrugator insertion point.48 Failure to treat the lateral corrugators can result in an irregular contraction pattern.12,31,48
Finally, when treating the glabellar complex, it is important to realize that splaying of the eyebrows may occur as a result of reduced inferomedial muscle movement, leading to change in facial appearance.48
4.3.3 Lateral Canthus
Lateral periorbital rhytids are a product of orbicularis oculi muscle contraction and, to a lesser extent, contraction of the zygomaticus major muscle. It is imperative to ascertain the relative contribution of each muscle in order to formulate an appropriate injection pattern. Similar to other areas, the deeper the dynamic lateral canthal lines (LCLs), the higher the dose generally needed. Additionally, the more extensive the area of involvement, the greater the number of injection sites required.
Diagnostically, the relative contribution from orbicularis oculi and zygomaticus muscles may be determined by having the patient make expressions that utilize different muscle groups. A big smile that includes cheek movement is caused by a combination of orbicularis oculi and zygomaticus major activity. In contrast, “squinting” as if in a sandstorm without cheek movement is mostly caused by orbicularis oculi movement. Thus, wrinkles in patients who have LCLs with a big smile but not with squinting are predominantly due to zygomaticus major muscle activity and, thus, they will have a suboptimal response to orbicularis oculi treatment. Conversely, if wrinkles are also present with squinting, it is expected that orbicularis oculi treatment will give significant improvement. Communicating this to the patient prior to treatment is paramount in achieving patient satisfaction.
The standard on-label injection pattern for LCLs consists of 4 units into each of three sites per side for a total of six injection points, and a total of 24 units of BTX-A or equivalent per point.40 The first lateral canthal injection should be placed at least 1 cm temporal to the lateral canthus in order to avoid diffusion to extraocular muscles and the palpebral portion of the orbicularis oculi which can result in strabismus and lid ptosis.
When treating the LCLs, injections should be superficial given that the orbicularis oculi muscle is thin. However, given that males have thicker skin, the depth of injection and dosing may need to be modified accordingly.28
In men who have more lateral extension of LCLs, an additional row of injections lateral to the first row may be considered.31 However, a consensus panel was divided on this approach.49 Those against it suggested addressing volume loss to treat elongated LCLs, whereas others encouraged the use of a second row of neurotoxin when significant sun damage and cosmetic surgeries, such as facelifts, were the suspected etiology.49
As noted earlier, men more frequently exhibit the downward fan LCL pattern. Even in these cases, three injection points are encouraged while paying attention not to venture medial to a vertical line drawn through the lateral canthus or lower than the maxillary prominence.30 Exercising caution when injecting the lower LCLs will help avoid inadvertent weakening of the zygomaticus major muscle, inability to raise the corner of the mouth when smiling, and a resultant asymmetric or “crooked” smile.
The authors note that naturalness of the smile is frequently overlooked when considering LCL treatment. In individuals with large cheeks, treatment of this area can lead to a shelflike appearance at the LCL–cheek junction consisting of anterior overprojection of the cheeks with a sudden stop at this junction and above which there is no projection, thus creating a linear demarcation between the two zones.50 To better understand this, reviewing the anatomy of this area is instructional. The zygomaticus major muscle originates from the lateral aspect of the zygomatic bone in the superior cheek region and runs inferomedially inserting at the angle of the mouth. It contributes to lifting of both the middle and superior cheek regions. The authors surmise that the shelflike appearance is caused by weakening of the superior portion of the zygomaticus major muscle with reduced ability to lift the uppermost part of the cheek. The upper noncontractile area appears flatter, in contrast to the contractile portion below which creates volume due to muscle activity, and which combined with the inability to lift the cheek beyond this point means that cheek volume can only move anteriorly. The resultant effect is a shelflike appearance with a line of demarcation separating the overly projected cheek inferior to the line and flattening above it.
These nuances must be addressed during the consultation process to ensure that realistic expectations are set.
4.3.4 Masseters
BTX-A use outside the upper face is less common in males.12,31 Important considerations when formulating a treatment plan include assessment of facial proportion and shape, especially the lower face, and the presence or absence of jowls. The patient should be examined both at rest and while clenching the teeth. If the facial shape is such that there is excess bulging at and above the mandibular angle and if the muscle is palpable with contraction, treatment may be indicated if a less square shape is desired. However, the presence of jowls or skin laxity may be a relative contraindication as treatment in these cases may lead to worsening of the jowls.
Generally speaking, because men typically prefer a square lower facial contour, treatment of the masseters to reduce muscle bulk is less commonly employed than in women, who often prefer a rounder contour. Having said that, masseter treatment has also been utilized to balance masseter asymmetry41 and in the treatment of bruxism.51,52 As with other areas, the larger the muscle mass, the higher the dose of BTX-A required. Injecting 1 cm lateral to the anterior border of the masseter muscle will help prevent inadvertent weakening of the risorius muscle and resultant smile asymmetry. Focusing injections on the lower half of the muscle is considered safest.53
A 20 to 50% higher dose than that used in females has been suggested.12 A consensus group recommended from one to five injection points per side consisting of 5 to 15 units of BTX-A or equivalent per injection point.49 Three to four injection sites per side is most common in our practice and we recommend titrating the dose so as to achieve the desired degree of muscle bulk reduction and facial contour. Typical total dosing is 15 to 40 units of BTX-A per side.
4.3.5 Other Facial Uses
A myriad of other BTX-A indications have been reported over the years. In the region of the lower eyelid, reduction of the lower eyelid “jelly roll” appearance by treating the hypertrophic orbicularis oculi muscle may be accomplished by injecting 2 to 4 units of BTX-A or equivalent approximately 3 mm below the ciliary margin in the midpupillary line.54,55 Additionally, it is possible to widen the aperture of the eye and create a more rounded appearance by injecting 0.5 to 1 unit intracutaneously per side in the midpupillary line. This results in lowering of the inferior ciliary margin and creation of “almond-shaped” eyes.49 We advise against treating the infraorbital region in cases of lower eyelid skin laxity and when there is delayed recoil when tugging on the lower eyelid skin and releasing it so as to avoid excessive scleral show and festooning.
In cases of LCLs that extend inferiorly to form fine, hyperdynamic “accordion” cheek lines, superficial injection of very low doses of dilute BTX-A has been used to improve the depth and extent of the lines.56 The number of units used varies widely with the area to be covered, but the underlying principle is to inject very low doses over a large surface area in a large volume of reconstitution so as to avoid weakening the zygomaticus muscles.
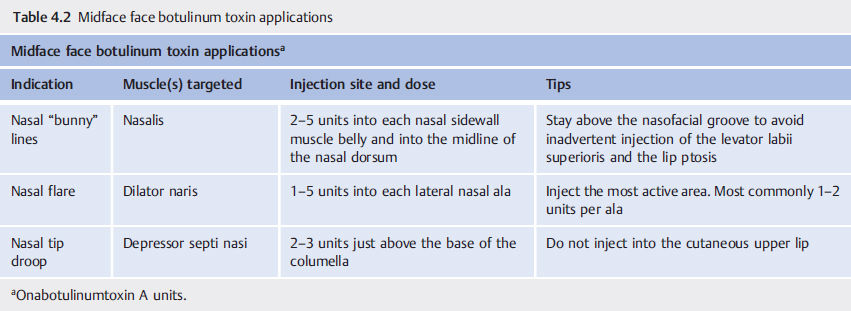
Usages in the midface include treatment of bunny lines, nasal flare, and nasal tip droop (Table 4.2). Bunny lines are treated by targeting the nasalis muscle and levator labii superioris alaeque nasi (LLSAN). The authors typically utilize one to two injection sites per proximal nasal sidewall and one in the proximal dorsal nose midline with total dosing between 6 and 15 BTX-A units. Nasal flare is treated by targeting the dilator naris muscle, the alar portion of the nasalis muscle, as well as the medial portion of LLSAN. One to 2 units of BTX-A in each mid-nasal ala are typically used. For individuals with nasal tip droop that is accentuated when enunciating “Peter” or “Bob,” nasal tip elevation may be achieved by targeting the depressor septi nasi muscle with 2 to 6 units of BTX-A just above the nasocolumellar junction.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


