Fig. 19.1
Hurley stage II characterized by recurrent nodules and abscesses, formation of sinus tracts, and scarring

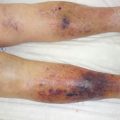
Fig. 19.2
Hurley stage III characterized by diffuse involvement of the area with multiple interconnected sinus tracts
Secondary lesions include cutaneous ulcerations, pyogenic granulomas, and hypertrophic scars, the latter appearing as indurated plaques or linearly ropelike scars. In contrast to closed comedones, which never occur in HS-affected areas, multiple, big, open comedones (the so-called tombstone comedones) may be seen in previously active areas.
Biopsies are rarely needed as the diagnosis is based on the clinical presentation; nonetheless, in some cases, differentiation from other skin diseases, such as pyoderma gangrenosum and cutaneous Crohn’s disease, might be difficult and require histopathological investigations. The characteristic histological findings include follicular hyperplasia and hyperkeratosis, local infiltration of inflammatory cells, formation of sinus tracts, and presence of necrosis. Microbiological examinations most frequently fail to identify pathogens.
19.3 Pathophysiology
The folliculopilosebaceous unit is the primary focus of the pathologic processes involved in hidradenitis suppurativa; however, the etiology remains controversial. Different theories have been proposed to explain the pathogenesis. These include the suggestion of an immune response dysfunction, as it has been proposed that the disease is a result of an inappropriate immunologic response to the normal skin flora, similar to the pathogenic processes involved in Crohn’s disease. Indeed, elevated levels of proinflammatory cytokines, including tumor necrosis factor-α and interleukin-1β, and involvement of the interleukin-12–interleukin-23 pathway have been shown [5]. Further, the lack of expression of human beta-defensin-2, an important antimicrobial peptide of the innate immune system against Gram-negative bacteria, in HS lesions supports this theory. However, the histopathological findings in early disease and investigations of basal membrane zone in the folliculopilosebaceous unit point towards a structural defect in the sebofollicular junction as the possible main cause [6]. It is hypothesized that mechanical trauma makes the structurally defect folliculopilosebaceous unit release keratin and other mediators, thereby triggering inflammation and inducing tissue destruction and necrosis.
The possibility of HS being a defect in wound healing has also been discussed. It has been hypothesized that whereas breaches of the follicular epithelium are common following infections or physical trauma, the perpetuation of the subsequent inflammatory process which could lead to HS is not. It may, therefore, be speculated that a disturbed wound healing process following the inflammatory stage occurs as a major factor in HS. This theory is supported by the detection of highly elevated levels of matrix metalloproteinase-2 in keratinocytes, fibroblasts, sweat glands, and hair follicles in lesional HS skin, indicating dysregulated tissue repair and reconstruction following unspecific tissue damage [7].
19.4 Treatment
Treatment of hidradenitis suppurativa is often a challenge [8]. By the time the diagnosis is made, most patients have been treated with short-term antibiotic regimens for several years without experiencing any effect, as the lesions are commonly misinterpreted as furunculosis or common abscesses. Establishing a strong alliance with the patient, attempting to restore the patient’s faith in the doctor-patient relationship and explaining the fluctuating nature of the disease are highly beneficial in minimizing the risk of low patient compliance. This is especially important in the case of resistant disease, where several therapeutic approaches might be carried out until the one or the combination inducing sufficient improvement is found.
Mild disease is often managed with topical therapy, such as topical clindamycin, or occasional intralesional glucocorticoid injections. However, in case of moderate to severe disease, topical agents are inadequate and systemic therapy usually indicated. Systemic treatment options include oral antibiotics with immunomodulatory properties such as tetracycline, doxycycline, clindamycin, and rifampicin; antiandrogenic therapies; and systemic immunosuppressive therapy, including tumor necrosis factor-α inhibitors [1].
In elements refractory to medical treatment and in the presence of scarred lesions, surgery, nonetheless, is a mainstay of therapy. Surgical approaches include exteriorization (“deroofing” of sinus tract, abscesses, and cysts [Fig. 19.3]) and surgical excision of lesional skin, with radical excisions being associated with lower recurrence rates. Alternatively, destruction of lesional hair-bearing skin is achieved using ablative CO2 laser [9]. The surgical and ablative laser approaches are based on the removal/destruction of the cutaneous structures involved in the disease, thereby causing open wounds requiring closure or management.