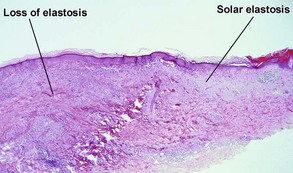
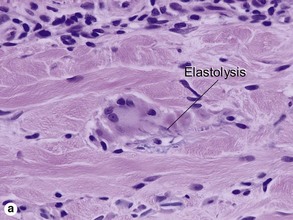
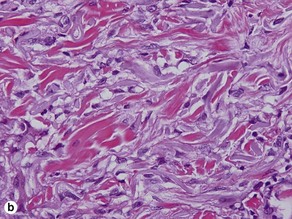
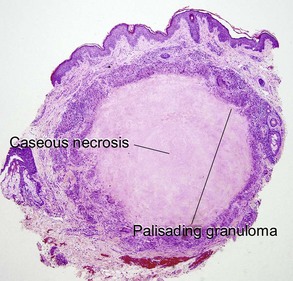
Chapter 10 Table 10.1 shows distinctions between granuloma annulare and necrobiosis lipoidica. Table 10-1 Features of granuloma annulare and necrobiosis lipoidica These lesions occur on areas of chronic sun damage such as the face, neck, hands, and arms. They have a raised border and atrophic finely wrinkled center. The granulomas consume actinically damaged elastic tissue. Other names have included Miescher’s facial granuloma, atypical necrobiosis lipoidica of the face and scalp, and annular elastolytic giant cell granuloma. Some consider it to be a variant of granuloma annulare on sun-damaged skin. The central loss of elastic tissue, absence of mucin, and conspicuous multinucleated histiocytes are the primary basis for distinguishing these lesions. A large proportion of patients with necrobiosis lipoidica have diabetes, thus the original name necrobiosis lipoidica diabeticorum. However, fewer than 1% of patients with diabetes have necrobiosis lipoidica. The pretibial area is the most common site but other areas of the lower extremities, arms, hands, and trunk can rarely be involved. The histology mimics subcutaneous granuloma annulare and rheumatic fever nodules. Rarely similar nodules occur in systemic lupus erythematosus.
Granulomatous and histiocytic diseases
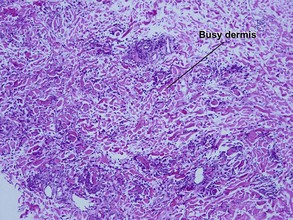
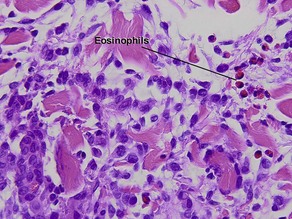
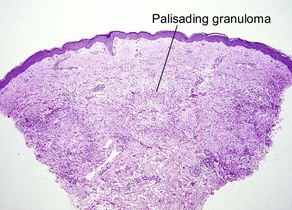
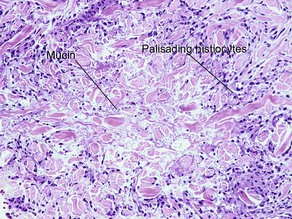
Granuloma annulare
Feature
Granuloma annulare
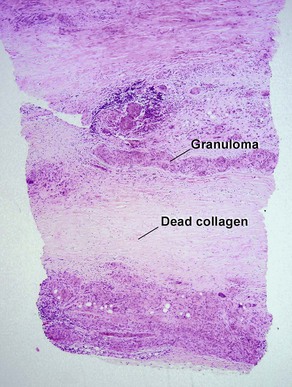
Necrobiosis lipoidica
Distribution
Focal and patchy
Diffuse and full-thickness
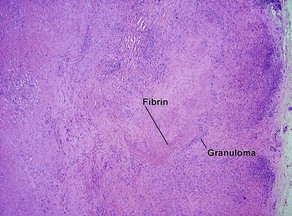
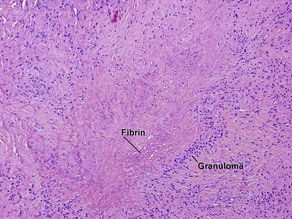
Granuloma
Palisaded or interstitial
Horizontal tiers (layers)
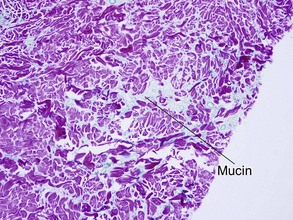
Mucin
Yes
No
Shape of punch biopsy
Tapered
Rectangular
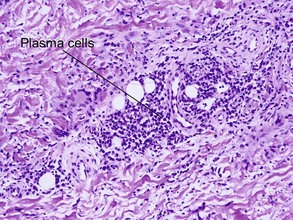
Plasma cells
Rare
Common
Cholesterol clefts
No
Occasional
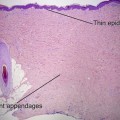
Actinic granuloma
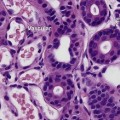
Necrobiosis lipoidica
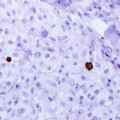
Rheumatoid nodule
Granulomatous and histiocytic diseases