14 Glabella/central brow
Summary and Key Features
• Soft tissue augmentation of the glabella and central brow is increasingly recognized as an important part of the pan-facial volumization strategy for many patients
• Augmentation of the glabella and central brow with fillers may be performed to correct age-related volume loss, or for the purposes of enhancement
• The glabella and central brow are anatomically unforgiving with regard to both safety and aesthetic considerations
• An understanding of anatomy and the physicochemical characteristics of fillers (including rheology) drives the selection of appropriate filler products and safe, efficacious injection techniques
• For many patients, the combination of fillers with neuromodulators will produce more a natural-looking rejuvenation than treatment with neuromodulators alone
• Fillers are also of value for patients with residual rhytides after neuromodulator treatment of the glabella and central brow
• A thorough pre-procedural consultation and discussion of realistic objectives are key to optimizing patient satisfaction
• Superficial or deep injection approaches may be employed alone or in combination. For both approaches, hyaluronic acid fillers may be the best option owing to their potential reversibility and excellent safety margin
• Meticulous sterile technique is essential before and during all filler injection procedures to minimize the risk of infection or biofilm.
• When properly performed, filler injections to the glabella and brow have a high rate of patient satisfaction and can profoundly improve the aesthetic appearance of the whole face
Epidemiology and patient selection
1. Patients with residual rhytides following neuromodulator injections. These patients, who generally have some degree of volume loss and decreased skin elasticity, can be identified in advance of neuromodulator injection to the glabella and central brow with a skin stretch test, and counseled at that time regarding the likely need for adjunctive filler. Filler can correct volume loss and compensate to some extent for loss of skin elasticity.
2. Patients who prefer to retain some degree of glabellar and central brow mobility after neuromodulator treatment. Neuromodulator dosing strategies for the glabella and forehead, including the central brow, vary depending on patient preference for a mobile versus a ‘frozen’ look. Patients who wish to retain maximum expressivity and avoid a ‘frozen’ look may be best treated with relatively low doses of neuromodulators to the glabella and forehead, including the central brow, plus adjunctive filler.
3. Patients with volume loss from the glabella and forehead, including the central brow. Glabellar volume loss often assumes the form of two parallel vertical furrows of variable depth. In the forehead including the central brow, volume loss may be focal or more general, respectively resulting in localized or more diffuse, trough-like concavities. Volume loss to the glabella is generally primary and age related. Volume loss to the central brow may also be primary, or secondary to neuromodulator-related atrophy of the frontalis. This is a thin sheet-like muscle and this author has observed anecdotally that it has a propensity to develop atrophic areas in some patients after repeated neuromodulator injections over many years, especially if these injections are of high dosage.
4. Patients desiring augmentation or enhancement of forehead / central brow convexity. There are individual and cultural / ethnic variations in the preference for a convex or even domed forehead. Forehead augmentation has become especially popular in Korea and other Asian countries. It is interesting to note that neuromodulator treatment of the upper face, the most popular non-surgical rejuvenative procedure in the USA, is rarely performed on patients in these countries because they do not tend to frown in the way that Caucasians do.
5. Patients who decline neuromodulator treatment but still wish to improve rhytides in the glabella and central brow regions.
Anatomical considerations
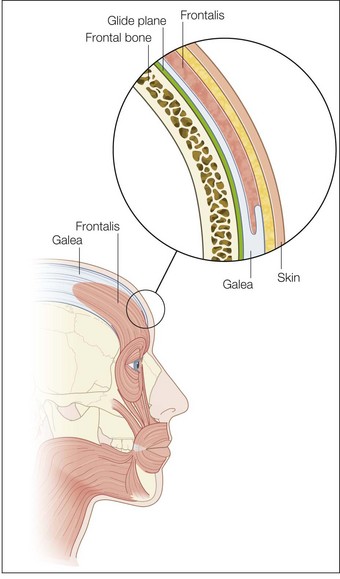
The most superficial tissue plane of the glabella and central brow is the skin, comprising the epidermis and dermis. Beneath this lies the subcutaneous tissue, then the superficial fascia, which covers the underlying muscles. There is loose subgaleal areolar tissue below the muscles, then the periosteum, which represents the deep fascia in this region and rests upon the bone (Fig. 14.1).
Decision-making: selection and preparation of filler product, selection of injection plane
General considerations
An understanding of structural and functional anatomy and of the physicochemical characteristics of fillers – including the flow-related (rheologic) properties of elasticity (G prime) and viscosity that predict their behavior – informs the selection of appropriate filler products and injection techniques to achieve optimal results (see Box 14.1, Tables 14.1 and 14.2; see also Figs 14.2–14.6).