Classical form of GCA, with involvement of the extracranial branches of the carotid artery
Early
Headache, jaw claudication, purpuric lesions and tender nodules in temporal region, temporal artery pain, temporal artery pulseless, weight loss, fever, visual manifestations, polymyalgia rheumatica (in 30–50 % of the cases) [5]
Late
Ulceration and/or gangrene of frontotemporal scalp or tongue
Early
Swelling, pain, claudication
Late
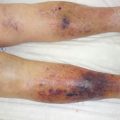
Ulceration, necrosis (Fig. 18.1), gangrene of the distal parts of the limbs
Major complications
Ischemic optic neuritis/blindness, stroke (mainly vertebrobasilar territory), aortic complications (aneurysms, dissection) [6]

Fig. 18.1
Vast ulceration and necrosis of the buttock due to giant cell arteritis in a 76-year-old female, with associated signs: jaw claudication, temporal artery pulseless, weight loss, visual manifestations, and amputations of the left forefoot weeks before. Improvement of the ulcerations of the seat after initiation of glucocorticoid therapy
(c)
Criteria (Table 18.1)
Table 18.1
ACR classification criteria for giant cell arteritis
Age ≥50 years at disease onset |
New onset of localised headache |
Temporal artery tenderness or decreased temporal artery pulse |
ESR ≥50 mm/h |
Biopsy: necrotising arteritis; mononuclear cell infiltrates or a granulomatous process with multinucleated giant cells |
Presence of ≥3/5: sensitivity of 93 % and specificity of 91 % for distinguishing GCA from other primary vasculitis syndromes |
(d)
Routine evaluation
Get Clinical Tree app for offline access

Biology
Elevated C-reactive protein (CRP), erythrocyte sedimentation rate (ESR)
Thrombocytosis
Anaemia
Abnormal liver function tests, particularly raised alkaline phosphatase
Raised α1 and α2 globulins on serum electrophoresis
No autoimmune disorders [2]
Histology
Temporal artery biopsy (TAB).
Recommended in all suspected cases.
Should be performed soon after the onset of treatment.
The sensitivity and specificity of TAB has been reported to be around 75 and 90 %, respectively.
Histological features: inflammation of the vessel wall by infiltration of T cells and macrophages, presence of giant cells, granulomatous lesions, intimal hyperplasia and destruction of elastic fibres, and arterial lumen partially or completely occluded.
Histologic signs of inflammation may be missed in TABs performed in arteritis-free segments because GCA affects vessels focally and segmentally.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree