, Teresa S. Wright2, Crystal Y. Pourciau3 and Bruce R. Smoller4
(1)
Department of Pathology & Immunology, Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas, USA
(2)
Departments of Dermatology and Pediatrics, University of Tennessee Health Science Center, Memphis, TN, USA
(3)
Departments of Dermatology and Pediatrics, Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas, USA
(4)
Department of Pathology and Laboratory Medicine, University of Rochester School of Medicine and Dentistry, Rochester, NY, USA
13.1 Toxoplasmosis
13.1.1 Clinical
Toxoplasmosis is a parasitic infection caused by the protozoa Toxoplasma gondii . Congenital infection usually results from transplacental transmission of protozoa after primary infection of a woman during pregnancy. Prevalence of congenitally acquired disease in the United States is 10 to 33 per 100,000 live births or 40 to 4000 cases per year [1].
Cutaneous lesions of congenital toxoplasmosis are variable, and include generalized morbilliform eruption, scarlatiniform eruption, subcutaneous nodules, and a “blueberry muffin ” rash characterized by scattered violaceous papules and nodules [2].
13.1.2 Histology
Toxoplasmosis only rarely involves the skin, and biopsies are seldom performed. The microorganisms can be present at any level of the epidermis, dermis, and subcutis [3, 4]. They may be present as pseudocysts or trophozoites within macrophages or in extracellular space in the dermis. The most common finding is that of a superficial and deep inflammatory infiltrate consisting of lymphocytes and histiocytes that is nonspecific and remarkable only for the presence of microorganisms [5]. A panniculitis reaction pattern, also specific only for the presence of toxoplasmosis, is also possible [6]. Less commonly, cases that have clinical and histologic features of a lichenoid dermatitis, graft vs. host disease, dermatomyositis, or erythema multiforme have been described [7, 8]. The presence of microorganisms within keratinocytes has also been described in an immunocompromised host [4]. In rare cases, pseudoepitheliomatous hyperplasia may occur.
13.1.3 Pathogenesis
Toxoplasmosis is caused by Toxoplasma gondii , a prevalent obligate intracellular parasite [9]. Infection occurs by ingestion of parasite cysts present in contaminated food or water [10]. The definitive host of T. gondii is cats, which can shed millions of sporozoites in their feces [11]. T. gondii tachyzoites can invade host cells, replicate, enter the circulation, and disseminate to multiple body sites [10]. T. gondii is found predominantly in macrophages shortly after infection [12]. The microorganism can cross the blood brain barrier by traveling inside parasitized leukocytes [13]. Toxoplasma induces chronic infection with tissue cysts persisting for the lifetime of the host .
13.2 Dermatophytosis
13.2.1 Clinical
Dermatophytosis refers to superficial fungal infections of the skin, hair, and nails. These infections are caused by dermatophyte fungi in three genera: Trichophyton, Microsporum, and Epidermophyton [14]. Dermatophytosis affects approximately 20–25 % of the world’s population and about 10–15 % of people are infected at some point in their lives [15]. Dermatophyte infections are generally named and classified by the affected anatomic locations, for example, tinea capitis for the hair and scalp (Fig. 13.1), tinea faciei on the face (Fig. 13.2), tinea manuum for the hands, tinea corporis for the body (Fig. 13.3), tinea cruris for the groin, tinea pedis for the feet, and tinea unguium for the nails. Majocchi’s granuloma is the name given to a similar fungal infection involving hair follicles (Fig. 13.4).




Fig. 13.1
Tinea capitis presents as scarring alopecia, pronounced scale and scattered erosions affecting the majority of the scalp in an infant treated with high potency topical steroids
Fig. 13.2
Tinea faciei is seen in a girl with multiple erythematous, scaly, annular plaques along the left side of the face
Fig. 13.3
Tinea corporis presents as adjacent erythematous, concentric annular plaques with scales
Fig. 13.4
Majocchi’s granuloma presents as a well-circumscribed, indurated, erythematous annular plaque studded with pustules
Erythematous scaly plaques that are annular or nummular in shape typically characterize dermatophyte skin infections. On the scalp, there is commonly associated hair loss and breakage. Sometimes there is significant inflammation with swelling and pustules. Affected nails are often thickened, discolored, and brittle. Treatment consists of topical or oral antifungal medications, depending on the location and severity of infection. Prognosis is generally good with appropriate therapy.
13.2.2 Histology
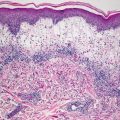
Histologic findings of dermatophytosis include parakeratosis and mild spongiosis with an underlying superficial perivascular lymphohistiocytic infiltrate (Fig. 13.5). Eosinophils are scant, and the infiltrate is mild in most cases. Small numbers of neutrophils and serum may be seen in the stratum corneum, usually adjacent to areas with parakeratosis. Onychomycosis demonstrates similar findings within the keratin of the nail plate [16]. In some cases, yeast and hyphal forms are readily apparent on routine H&E sections, while in other cases, Periodic acid–Schiff stains with diastase are very helpful in highlighting the microorganisms. While some authors have advocated pretreating histologic sections with NaOH as a means of enhancing detection, this technique is not currently widely practiced by pathologists [17]. Histologic changes are essentially independent of the inciting species of dermatophyte or the site affected [18]. In some cases, the fungi are pigmented, giving rise to tinea nigra (Figs. 13.6 and 13.7). This fungal pigmentation is easily observed on routine histologic sections.
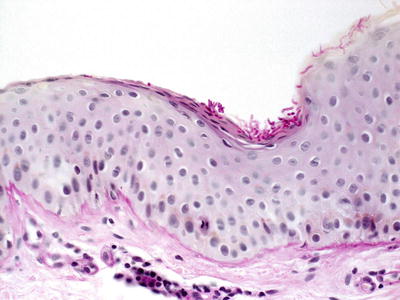

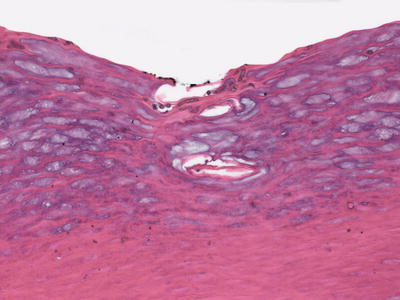
Fig. 13.5
Dermatophytes are present within the stratum corneum, often adjacent to foci of parakeratosis. Inflammation is variably present. Spores and hyphae are visualized with Periodic acid–Schiff stains
Fig. 13.6
Tinea nigra presents as a well-circumscribed, round, brown patch with dry scale along the medial aspect of the foot in a young boy
Fig. 13.7
Tinea nigra demonstrates pigmented yeast and hyphal forms in hyperkeratotic stratum corneum on acral skin
Dermatophytes involving hair follicles in the scalp result in suppurative folliculitis, in which case the inflammatory infiltrate is much more pronounced and may include abundant dermal neutrophilic abscesses [19]. In florid and long-standing cases, dense dermal scarring with pronounced alopecia may occur [20]. In children, tinea capitis is the most common presentation of folliculo-centric dermatophytosis. Majocchi’s granulomas also occur in children [21]. In cases of kerion or Majocchi’s granuloma, fungal organisms are present within the keratinaceous portions of the pilosebaceous structures. Microorganisms are not ordinarily found in the dermis despite the brisk inflammatory response secondary to follicular rupture.
The histologic findings of tinea capitis include inflammation within and around follicular epithelium, with or without involvement of the overlying epidermis. Depending upon the severity of the process and the acuity of the condition, the inflammation may be predominantly neutrophilic with abscess formation within hair follicles, or may consist of a less intense lymphocytic infiltrate. In florid cases, rupture of the follicular epithelium may result in a granulomatous response with neutrophils and abundant multinucleated giant cells. Fungi may be identified with routine H&E staining, but they are highlighted and easily visible on a Periodic acid–Schiff stain using diastase or a methenamine silver stain [22]. Tinea capitis is primarily caused by Microsporum canis or Trichophyton tonsurans which can be confirmed with fungal cultures [20, 23]. Majocchi’s granuloma can occur in children. It is a suppurative fungal-induced folliculitis. Histologic findings demonstrate neutrophilic abscesses primarily within follicular structures. Abscesses may extend into the surrounding dermis, and result in a suppurative process throughout the dermis [19]. As hair follicles rupture, a granulomatous response is seen with abundant multinucleated giant cells admixed with a dense neutrophilic infiltrate [21]. Extension into the subcutaneous fat is not uncommon. Frequently, there are epidermal hyperplasia, parakeratosis and neutrophilic abscesses within the stratum corneum. With chronic infection, dermal fibrosis and distortion of the follicular architecture may develop [19].
13.2.3 Pathogenesis
Dermatophytes can survive solely on the outer stratum corneum layer of the skin [24]. Studies have shown that dermatophytes require about 6–12 hours to adhere to the host tissue, 16 hours to germinate, and 72 hours to invade into the stratum corneum [25, 26]. Once they adhere to keratinized tissue, dermatophytes release enzymes, such as keratinases, metalloproteases and serine proteases, as well as lipases and ceramides. These enzymes cleave proteins and lipids in keratinized tissue and induce an inflammatory response, resulting in tissue injury [27, 28]. Infections by dermatophytes generally induce a type 1 T-helper cell response with the production of interleukin-2 and interferon-γ [28]. The production of antibodies is also important in the overall immune response to dermatophytes. In acute fungal infections, cellular-type immune response predominates, whereas in chronic fungal infections, antibody-mediated response, involving mainly IgE and IgG, is the primary reaction [26].
In tinea capitis, fungal hyphae grow in the stratum corneum and the hair follicles, extending upward as the hair grows [29]. Endothrix infection occurs when arthroconidia (spores) are present in the hair shaft. In tinea capitis, there is severe inflammation leading to subcutaneous pustule formation and hair loss. Th17, a type of CD4-positive helper T cells, may have a role in the pathogenesis. Increased number of circulating Th17 cells have been reported in a patient with tinea capitis [30].
Majocchi’s granuloma results from chronic dermatophyte infection of the skin or nails that eventually disseminates into the dermis and subcutaneous tissue. Predisposing factors that affect cell-mediated immunity and the inflammatory response include long-term use of steroids, chemotherapy, and immunosuppressive drugs [21, 31]. Dermatophyte infection induces toll-like receptor (TLR) -mediated activation of keratinocytes and monocytes that can inhibit a number of antimicrobial peptides, such as cathelicidins, which are important in skin defense mechanisms against pathogens [32]. Neutrophils and macrophages are crucial for the control of invasive fungal infections by ingesting and killing fungal spores and hyphae [33]. Type 1 T-helper cell (Th1)-mediated immunity is important in dermatophytic infections [21, 34]. Immunosuppressive therapy that impairs cellular immunity can result in generalized Majocchi’s granuloma.
The physical barrier integrity of the skin is important in the pathogenesis of Majocchi’s granuloma. Factors that impair the barrier integrity, such as physical trauma, can lead to hair follicle disruption and entry of microorganisms from the epidermis into the dermis. Keratinous materials that are introduced into the dermis after follicular disruption can potentially provide proteinaceous substrates for the survival of dermatophytes [35, 36]. Changes in the dermal milieu due to fungal infection may create a favorable environment for fungal pathogens to survive and grow .
13.3 Candidiasis
13.3.1 Clinical
Congenital cutaneous candidiasis is defined as widespread cutaneous candida infection that typically presents within the first 6 days of life. Up to 25 % of pregnant women harbor Candida albicans in their vaginal flora, and mucocutaneous candida infection is fairly common in infants. However, congenital cutaneous candidiasis is relatively uncommon with few confirmed reports in the literature [37].
Affected infants may have cutaneous involvement alone or serious systemic infection with respiratory distress and even sepsis [37]. The most common clinical presentation is a generalized eruption consisting of small erythematous macules, papules, and pustules which resolves without serious sequelae (Fig. 13.8) [38]. Approximately half of affected infants respond well to topical antifungal therapy. The majority of infants have a benign course with complete recovery.

Fig. 13.8
Erythematous thin plaques are present at the mons pubis, labia majora, and medial thighs with satellite papules and pustules in irritant contact diaper dermatitis with superimposed candida
13.3.2 Histology
Histologic findings in cutaneous candida infection are those of a pustular dermatosis. Within the epidermis, there is focal spongiosis with neutrophils extending from the superficial dermis into the epidermis, and frequently forming subcorneal pustules (Fig. 13.9). The dermis is relatively uninvolved with only scattered superficial neutrophils admixed with lymphocytes and occasional eosinophils. Diagnosis is confirmed on Periodic acid–Schiff stains with diastase that demonstrate abundant yeast forms. Candidiasis can also be seen in biopsies taken from nails, in which cases the microorganisms are found within the nail keratin with neutrophils and serum deposition [39]. Invasive candidiasis is encountered in severely immunocompromised hosts. Microorganisms can be present in great abundance in the dermis or in blood vessels with candidal septicemia [40].
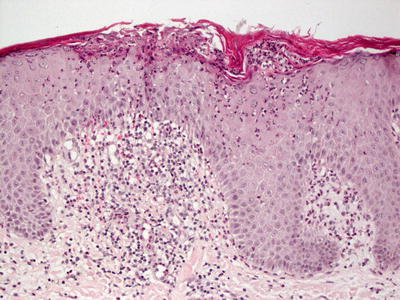
Fig. 13.9
Candida infection of the skin shows subcorneal neutrophilic abscesses with inflammation of the underlying dermis
The differential diagnosis includes other subcorneal pustular dermatoses, including psoriasis, acute generalized exanthematous pustulosis, pustular dermatophytic infections, some cases of IgA pemphigus, infantile acropustulosis, and transient neonatal pustular melanosis. The clinical history and special stains for microorganisms make the distinction relatively straightforward [41].
13.3.3 Pathogenesis
Candida albicans is a dimorphic fungus that can colonize a variety of tissues, including the skin and oral and vaginal mucosa. Competing commensural bacteria and the local host immune response prevent an overabundance of Candida [42]. When the normal flora is altered by antibiotic treatment or in immunocompromised states, the result can be an overgrowth of Candida, such as candidiasis on mucosal surfaces (thrush).
Recognition of Candida by the host immune system requires toll-like receptor (TLR) 2 and Dectin-1 on immune cells [43–45]. The NLRP3 (NACHT, LRR, and PYD domain-containing protein) inflammasome is important in the host immune response to fungal infection. NLRP3 inflammasome is associated with interleukin-1 response to a variety of pathogens, including Candida albicans [46]. Dendritic cells are important in the host immune defense against Candida. Dendritic cells phagocytoze the yeast form of Candida albicans and induce the differentiation of CD4+ T lymphocytes into type 1 T helper cells (Th1 cells) and the activation of B lymphocytes and the maturation of phagocytic cells [47, 48]. Among the cytokines involved in Candida infection, IL-33, which induces a type 2 T helper cell (Th2) inflammatory response and activates both innate and adaptive immunity, has a pivotal role in the host immune defense against fungal pathogens [48].
13.4 Chronic Mucocutaneous Candidiasis
13.4.1 Clinical
Chronic mucocutaneous candidiasis is seen in a variety of disorders in which patients experience persistent or recurrent Candida albicans infections of the mucous membranes, skin, and nails. Some of these conditions are inherited or associated with primary or secondary immunodeficiency [49]. Infants often present with persistent oral thrush and candida diaper dermatitis. Over time, they develop more widespread erythematous, scaly plaques, especially on the scalp and extremities. Occasionally, these plaques develop into thick granulomas. Nails may become thick, dystrophic, and discolored [50]. Most patients require systemic antifungal medications for disease control.
13.4.2 Histology
Histologic changes in chronic mucocutaneous candidiasis resemble those seen in acute candida infections. Subcorneal pustules, mild epidermal spongiosis, and the presence of yeast forms and pseudohyphae are seen. The microorganisms may be apparent on routine H&E sections, but they are better visualized on Periodic acid–Schiff stains [51]. In long-standing lesions, psoriasiform epidermal hyperplasia is present. In some patients, a granulomatous dermal infiltrate is seen, and microorganisms may be present within the granulomas [52]. Microorganisms are identified within affected nail plates [53].
13.4.3 Pathogenesis
Chronic mucocutaneous candidiasis affects patients with immunodeficiency, most commonly individuals with defects in the T-cell compartment, and those with diverse genetic defects that result in impaired IL-17 and IL-22 immunity [54]. Chronic candida infections during infancy serve as an indicator of primary immunodeficiency [55].
Signaling pathways associated with IL-17+ T helper cells (Th17) are important in immunodeficiency syndromes associated with chronic mucocutaneous candidiasis [56]. Mutations in CARD9, STAT3, IL17RA, IL17F, STAT1, and IL12RB and polymorphisms in Dectin 1 and interleukin-22 (IL-22) that cause impairment of function of Th17 cells are associated with the disease [57]. Studies have suggested that IL-17A- and IL-17F-producing cells are important Th17 cells in the host immune response against Candida.
Neutrophils are important in acute mucosal defense against C. albicans by preventing fungal dissemination [58]. Neutrophil mobilization and trafficking are induced in an IL-17RA-dependent manner [59]. IL-17 can induce the expression of antimicrobial peptides (AMPs) , including S100A8 and S100A9 (which form the heterodimeric complex calprotectin), β-defensin 3 and lipocalin 2. These molecules have direct antifungal activities through membrane depolarization and depriving the fungus of essential metal ions [60]. In patients with chronic mucocutaneous candidiasis, gain-of-function mutations in STAT1 shift the cellular response toward Th17 cell-inhibiting cytokines. Th17 cells secrete IL-17 and IL-22, which are cytokines with potent antifungal properties that induce the production of antimicrobial peptides and activation and recruitment of neutrophilsto mediate microbial killing. Mutations in IL17F and IL17R in patients with chronic mucocutaneous candidiasis, as well as neutralizing autoantibodies against IL-17 and IL-22 in patients with autoimmune polyendocrinopathy–candidiasis–ectodermal dystrophy can directly impair IL-17 and IL-22 immunity .
13.5 Blastomycosis
13.5.1 Clinical
Blastomycosis is caused by the dimorphic fungus Blastomyces dermatitidis . In the United States, annual incidence of blastomycosis is estimated at 0.3–1.8 cases per 100,000 people [61]. The typical patient with blastomycosis is a middle-aged man who spends significant time outdoors [62]. Blastomycosis is rare in children and adolescents. The majority of patients with blastomycosis have primary pulmonary involvement. Sometimes there is hematogenous spread of infection to extrapulmonary sites. Rarely, primary infection is acquired via cutaneous inoculation [63]. Skin involvement has been reported in 40–80 % of blastomycosis cases [62, 63]. Typical skin lesions appear as verrucous nodules and plaques or ulcerative lesions with raised borders. Therapy consists of systemic antifungal medication. Most patients with localized cutaneous disease have a favorable prognosis.
13.5.2 Histology
The histologic findings of blastomycosis in children are the same as those described in adults. The epidermis typically demonstrates pseudoepitheliomatous hyperplasia. Neutrophilic abscesses are present within the stratum corneum, epidermis, and dermis [64]. Foci of granulomatous inflammation can also be seen. Microorganisms are present mainly within the dermis, and they can be identified on routine H&E sections and highlighted with Gomori methenamine silver and Periodic acid–Schiff stains (Fig. 13.10). Blastomyces are broad budding yeasts with capsules that are approximately 6 μm in diameter. Microorganisms can also be detected on Tzanck smears, but this is not the normal method for establishing the diagnosis [65].
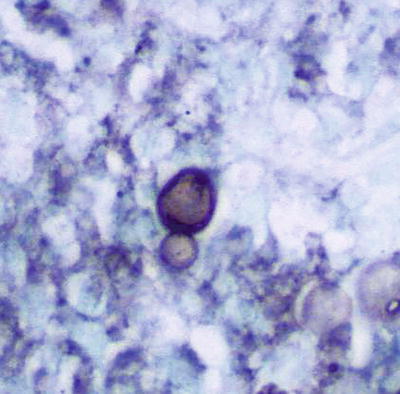
Fig. 13.10
Gomori-methenamine silver stain demonstrates the broad-based budding yeasts seen in blastomycosis
The differential diagnosis includes other deep fungal infections that cause pseudoepitheliomatous hyperplasia , such as chromomycosis and sporotrichosis. Tuberculosis, especially lupus vulgaris, may have similar histologic features, but it can be distinguished on acid-fast bacilli stain. Blastomycosis-like pyoderma, which is caused by bacterial infection, can induce pseudoepitheliomatous hyperplasia, but it is differentiated on special stains for microorganisms [66, 67]. Halogenodermas may be considered, but these typically contain abundant eosinophils within the dermis. Keratoacanthoma-type of squamous cell carcinoma may also demonstrate similar histologic features, but it is quite rare in the pediatric population .
13.5.3 Pathogenesis
Blastomycosis is caused by Blastomyces dermatitidis , which is a dimorphic fungus that causes systemic granulomatous disease [68]. The infection is prevalent in North America, most notably in the Ohio and Mississippi river valleys, and in some countries in Africa (such as Zimbabwe and South Africa) [69]. Infection by Blastomyces often originates in the lungs by inhalation of conidia of the fungus with secondary systemic spread via the lymphatics to other anatomic sites [70]. The most frequent site of dissemination of pulmonary blastomycosis is the skin (40–80 % of the cases), followed by bone (10–50 %), genitourinary tract (10–30 %), and central nervous system (1–5 %) [71]. Blastomyces can infect both immunocompetent and immunocompromised hosts. Studies have shown that 25 % of patients with blastomycosis have an immunocompromised status, such as diabetes mellitus, HIV, and malignancies [72].
13.6 Sporotrichosis
13.6.1 Clinical
Sporotrichosis is an infection caused by the dimorphic fungus Sporothrix schenckii . Although there is a pulmonary form of sporotrichosis, most infections are limited to the skin and subcutaneous tissues, and occur via direct inoculation following a puncture wound or skin abrasion [73]. The majority of individuals affected are males between the ages of 20 and 50 years old [74]. Although sporotrichosis can occur in children, it is relatively uncommon.
Clinically, there are three cutaneous patterns of sporotrichosis : fixed cutaneous, lymphocutaneous, and multifocal or disseminated cutaneous. In fixed cutaneous disease, a single papule forms at the site of inoculation, and develops into a crusted or verrucous plaque. In lymphocutaneous disease, an ulcerated nodule develops at the inoculation site, followed by the development of a string of similar nodules overlying the proximal lymphatic vessels. Multifocal disease is the least common disease presentation, and it refers to the development of three or more lesions appearing at two or more different anatomical locations. Although lymphocutaneous disease is the most common variety, accounting for 70–80 % of all reported cases, children are more likely to present with solitary lesions often located on the face [74, 75].
13.6.2 Histology
Sporotrichosis demonstrates pseudoepitheliomatous hyperplasia overlying a suppurative and granulomatous dermatitis (Figs. 13.11 and 13.12). Abundant neutrophilic abscesses are present along with caseating granulomas, multinucleated giant cells, histiocytes, and other inflammatory cells. The inflammatory process is diffuse throughout the dermis, and can involve the subcutis. The microorganisms are found in variable numbers of cases, and they are more readily identified in areas adjacent to caseating granulomas [76, 77]. Cases in which there are more epithelioid granulomas and a lymphocytic predominance tend to have fewer numbers of microorganisms [78]. Asteroid bodies are present in the great majority of cases, and microorganisms are frequently associated with these structures with spores ranging from 2 to 6 μm in diameter. They are most easily identified on Periodic acid–Schiff stains [79].
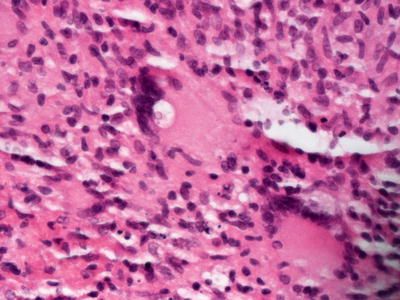
Fig. 13.11
Sporotrichosis demonstrates pseudoepitheliomatous hyperplasia and a dense inflammatory dermal infiltrate with granulomas
Fig. 13.12
Abundant granulomas , multinucleated giant cells, and intracellular organisms are present in sporotrichosis
The differential diagnosis includes cutaneous tuberculosis, particularly the lupus vulgaris variant with concomitant pseudoepitheliomatous hyperplasia. Acid-fast bacilli stains help to distinguish tuberculosis from sporotrichosis. Other deep fungal infections, such as chromomycosis and blastomycosis, can be distinguished based upon the morphology of the fungi. Halogenodermas do not tend to have caseating granulomas, and they are characterized by abundant eosinophils, which are not typically seen in sporotrichosis .
13.6.3 Pathogenesis
Sporotrichosis is an endemic disease caused by Sporothrix schenckii , a dimorphic fungus [80]. The fungal conidia usually enter the host by skin trauma and implantation of fungal microorganisms in the skin. The infection may extend deeply, involving the subcutaneous tissue, muscles, and fascia .
13.7 Chromoblastomycosis (Chromomycosis)
13.7.1 Clinical
Chromoblastomycosis is a chronic fungal infection of the skin and soft tissues. It is a result of traumatic injury to the skin followed by direct inoculation with fungal microorganisms [81]. Most patients with chromoblastomycosis are males between 50 to 60 years of age. Infection is uncommon in children [82]. Lesions commonly occur on the legs.
Clinically, five different presentations have been described: (a) nodular, where single or multiple pink to purple nodules are present; (b) tumoral, where larger nodular masses occur; (c) verrucous, where lesions have hyperkeratosis; (d) plaque, where there is one or more red to purple scaly plaques; and (e) cicatricial type, where there are large annular lesions with atrophic scarring [81]. Treatment is often difficult with low cure rates and high incidence of relapse [81]. However, systemic antifungal therapy, cryotherapy and thermotherapy, as well as surgical excision for limited lesions, have been tried with some success.
13.7.2 Histology
Chromoblastomycosis represents infection by one of a group of dematiaceous pigmented fungi [83]. Pseudoepitheliomatous hyperplasia is present and may be pronounced (Fig. 13.13). Fibrosis appears as the lesions become chronic [88]. In long-standing cases, transformation to squamous cell carcinoma has been reported [84–86]. As this transformation can take 10–20 years, it is not seen within the pediatric population. Within the dermis, there is a florid and diffuse granulomatous and neutrophilic inflammatory infiltrate. Neutrophilic abscesses can extend into the epidermis, and may be keratolytic. Brown yeast forms, ranging in size from 5 to 12 μm, are identified and appear as “copper pennies” [87] (Fig. 13.14). They may be present in both the epidermis and dermis [88]. These fungal elements are also known as “sclerotic bodies”. Ultrastructural examination demonstrates that microorganisms are directly engulfed by neutrophils [89]. While microorganisms can be identified on Periodic acid–Schiff stains, in most cases, they are readily apparent on routine H&E sections due to their characteristic brown color [90]. A rare cystic variant has been reported, in which microorganisms are confined to a cystic cavity within the dermis [91].
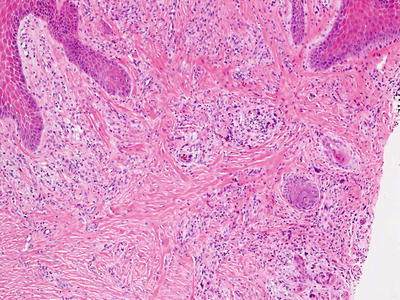
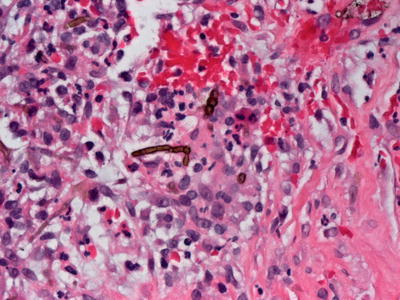
Fig. 13.13
Chromoblastomycosis demonstrates epidermal hyperplasia and mixed, focally granulomatous dermal infiltrate
Fig. 13.14
Pigmented spores and hyphae are present within histiocytes and in the dermis in chromoblastomycosis
The histologic differential diagnosis includes other disease entities that induce pseudoepitheliomatous hyperplasia, including sporotrichosis and blastomycosis. The presence of pigmented fungi makes the distinction straightforward. Halogenodermas do not contain fungi, often have many eosinophils, and can be distinguished based upon clinical history. Blastomycosis-like pyoderma demonstrates bacteria and does not contain dermal fungi .
13.7.3 Pathogenesis
Chromoblastomycosis is defined as a chronic fungal infection of the skin that typically develops after traumatic injury and inoculation of fungi into the skin. The causative agents are three fungal species: Fonsecaea pedrosoi , Phialophora verrucosa , and Cladophialophora carrionii [92]. F. Pedrosoi and C. carionii are the most common responsible agents in the USA [93]. These saprophytic fungi live on plants or vegetable debris in the soil. The characteristic dark, thick-walled cells (Medlar bodies) are present in chromoblastomycosis.
Neutrophils and macrophages are important cells in the immune response in chromoblastomycosis. Dermal macrophages and dendritic cells are antigen-presenting cells that present fungal antigens to lymphocytes. In response to fungal spores, dendritic cells produce TNF-α, IL-10, and IL-12 [81]. CD4+ T lymphocytes play an important role in chromoblastomycosis by producing IFN-γ in response to the microorganisms [94, 95]. Additionally, stimulation of the Toll-like receptor (TLR) pathway is important for activation of the adaptive immune response to chromoblastomycosis .
13.8 Coccidioidomycosis
13.8.1 Clinical
Coccidioidomycosis is an infectious disease caused by Coccidioides immitis , which is considered to be endemic in the Southwestern United States, with an annual incidence of approximately 150,000 cases [96].
Rarely, C. immitis may cause a primary inoculation infection at a site of skin trauma. This will typically result in a localized ulcerated plaque that heals over several months. More commonly, C. immitis causes pulmonary infection after the spores are inhaled. At least 60 % of individuals with acute pulmonary infection have no symptoms or only a mild respiratory illness [96, 97]. During this acute illness, patients may experience a generalized morbilliform skin eruption [98]. Approximately 5 % will develop erythema nodosum or erythema multiforme [99]. Symptomatic disseminated extrapulmonary disease develops in approximately 1 in 200 infected individuals [97]. Skin manifestations in disseminated extrapulmonary disease include multiple verrucous papules and plaques.
Most patients with primary infection recover spontaneously. However, patients with disseminated disease are treated with systemic antifungal therapy. Patients who are pregnant or immunocompromised are particularly vulnerable to severe, aggressive infection .
13.8.2 Histology
Histologic sections demonstrate variable degrees of epidermal hyperkeratosis and pseudoepitheliomatous hyperplasia (Fig. 13.15). Within the dermis, there is a marked granulomatous and suppurative inflammatory infiltrate with large microorganisms that contain endospores [100] (Fig. 13.16). Some cases display a predominance of neutrophils with extensive necrosis within the inflammatory infiltrate, while other cases develop more prominent granulomas and appear less suppurative. A third reaction pattern characterized by a proliferation of small dermal blood vessels and a vasculitic pattern has also been described [101]. Microorganisms can be found in most cases on H&E sections, but can be highlighted with periodic acid Schiff stains. Coccidioidomycosis immitis form spherules that measure from 10 to 80 μm in diameter, and contain abundant 2–5 μm endospores.
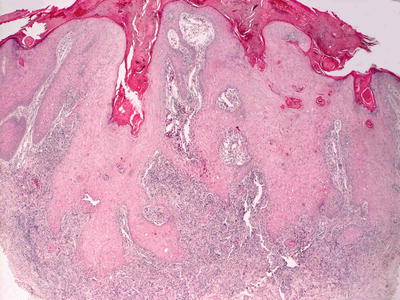
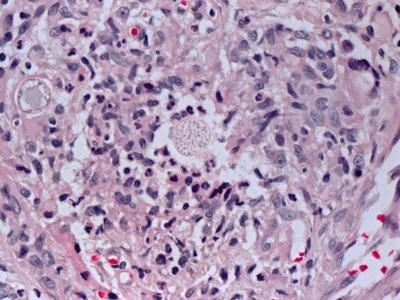
Fig. 13.15
Pseudoepitheliomatous hyperplasia is seen in some cases of coccidioidomycosis . There is a dense and mixed inflammatory infiltrate present in the dermis
Fig. 13.16
Large morules containing endospores are present surrounded by granulomatous inflammation in coccidioidomycosis
13.8.3 Pathogenesis
Coccidioidomycosis (also known as valley fever) is caused by two species of fungi, Coccidioides immitis and C. posadasii [105]. C. immitis is a fungus found in the soil in southwestern USA, while C. posadasii is found predominantly in South America. Immunosuppressive states and underlying autoimmune diseases are predisposing conditions for the activation of underlying Coccidioides infection.
Infection by arthroconidia elicits an innate immune response involving neutrophils [106]. Toll-like receptor-2 and Dectin-1 are necessary to trigger an innate immune response to fungal microorganisms [107]. Soluble factors derived from the fungus generate complement components that attract neutrophils, which phagocytose fungi [108]. Coccidioides bind to human peripheral monocytes and dendritic cells through the mannose receptor [109, 110]. Fungal arthroconidia can stimulate macrophages to produce tumor necrosis factor-α, interleukin-1β and interleukin-6 [111]. Type 1 T-helper cell response is important in host defense against Coccidioidomycosis with current research for treatment on identifying T cell antigens capable of inducing such type 1 immune response [112].
13.9 Histoplasmosis
13.9.1 Clinical
Histoplasmosis is an infectious disease caused by the dimorphic fungus, Histoplasma capsulatum . Most cases of histoplasmosis are limited to only pulmonary involvement. Skin involvement is uncommon, but it is estimated to occur in approximately 4–11 % of patients who develop disseminated disease [113]. Rarely, primary inoculation disease can occur after trauma to the skin.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


