9.2 Classification of Frostbite
There are a number of ways one can classify frostbite injuries, and the most commonly utilised classification is simply one of mild or severe injury, but the first predictive outcome classification was suggested by Cauchy et al. 2001 [3]. Cauchy’s classification is based on anatomical location, radiotracer uptake on technetium scanning and skin blistering. This was based on a retrospective study of 70 frostbite patients presenting to the Department of Mountain Medicine in Chamonix, France (Table 9.2).
Table 9.2
Predictive classification of frostbite injuries affecting the limb extremities
Severity grade | Lesion location (day 0) | Radioactive tracer uptake on bone scan (day 2) | Character of blistering (day 2) | Likely outcome |
|---|---|---|---|---|
1. | Not visible | N/A | None | No tissue loss or long-term sequelae |
2. | Distal phalanx | Hypo-fixation | Clear | Soft tissue loss with nail changes |
3. | Mid-phalanx | Absence of uptake at phalanx | Haemorrhagic | Amputation of digit. Functional sequelae |
4. | Carpus/tarsus | Absence of uptake at carpus/tarsus | Haemorrhagic | Extensive amputation with likely sepsis or thrombosis. Functional sequelae |
9.3 Pathology
A frostbite injury results both from the direct and indirect effects of freezing and pathologically is characterised by a continuum of overlapping pathological phases that ultimately cumulate in cellular ischaemia and necrosis of the affected tissues. These phases can be broadly divided into the following:
Pre-freeze phase
Freeze-thaw phase
Vascular stasis phase
Late ischaemic phase
9.3.1 Intracellular Effects
The direct effects of freezing are principally due to the formation of ice crystals within the tissues themselves. These crystals increase the oncotic pressure within the extracellular space, dehydrating cells via the osmotic movement of water out of the cellular membranes and disturb the intracellular homeostasis. With the rewarming of tissues, the crystals melt producing interstitial tissue oedema. Indirectly the freezing injury stimulates the release of a variety of pro-inflammatory cytokines.
9.3.2 Extracellular Effects: The Freeze-Thaw-Refreeze Injury
Initial exposure to cold temperatures results in an immediate, localised vasoconstriction. This may sometimes be followed by a transient vasodilatory reflex known as the “hunting response”, or cold-induced vasodilatation. This physiological reflex results in a redistribution of flow from the core and is thought to be a primitive reflex to protect the extremities from freezing. Ultimately this results in a drop in core body temperature and furthermore is ineffective in protecting the peripheries against extreme cold stress. The reduced blood flow secondary to vasoconstriction in turn further exacerbates localised cooling producing a vicious cycle of ever-increasing vasoconstriction and tissue cooling. An oedematous state results through a combination of increased plasma viscosity, microvascular damage and fluid migration. The microvascular (endothelial) damage produces a pro-thrombotic environment through activation of the clotting cascade in which microthrombi form, occluding the capillaries, resulting in ischaemia. When such a time as tissue rewarming occurs, further microvascular clot occlusion occurs due to the promotion of a pro-thrombotic state through the lysis of frozen cells. Local mast cells degranulate in response to the lytic cell membranes, releasing histamine which further increases vascular permeability and oedema. The end point of all of these processes is potentially devastating local tissue ischaemia, and as first noted by Baron Larrey, Surgeon General to Napoleon, the most significant ischaemia, and therefore tissue necrosis, is seen in injuries that freeze, thaw and are then frozen again.
9.3.3 Long-Term Sequelae
It should also be appreciated that aside from these immediate-type effects seen following a freezing injury, there is also long-term pathological damage sustained by tissues which may result in chronic dysfunction or impact upon the patient many years post-injury. Although rare, one of the most serious observed syndromes is probably related to chronic vasomotor dysfunction, manifesting clinically as chronic pain affecting the previously frostbitten area that is often unresponsive to conventional analgesia and requires anaesthetic or pain specialist input. Those that develop these complex regionalised pain syndromes frequently also suffer with associated problems such as paraesthesia and cold intolerance. It should also be noted that all patients who have experienced frostbite are at increased risk of further future episodes (presumably again secondary to vasomotor dysfunction) and all patients must be warned of this and given appropriate preventive advice. More serious long-term sequelae of frostbite that have been reported include the malignant transformation of frostbitten tissues and bone and joint pathologies including osteoporosis and arthritic changes [1].
9.4 Clinical Evaluation of Frostbitten Patients
9.4.1 History
Critical details of the patient history include the likely temperature, duration and timing of exposure, as this will help predict the severity of injury and may affect subsequent management. It is also important to obtain information relating to the patient’s premorbid state such as peripheral vascular disease and pertinent risk factors such as smoking or the use of β-blockers.
9.4.2 Examination
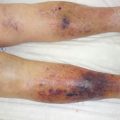
In rare cases frostbite injuries may present as a purely uniform frozen injury, but more frequently there is a mixed clinical picture with overlapping areas between deeper frozen tissues and more superficial nonfrozen tissues. Even in the case of a purely frozen injury, there is much variation in severity from the lesser affected forms (frostnip) to large areas of frozen tissues or indeed whole limbs.
It can be seen that frostbite presents in variable fashions and the injury evolves with time, and thus one is often unable to determine the full or likely extent of injury for some time after the injurious cooling from clinical examination alone, illustrating the importance of a thorough history. Nonfreezing injuries may be managed locally without the need for specialist intervention, and they typically follow a short exposure to (relatively) warmer temperatures and involve the feet most commonly with patients complaining initially of localised numbness and or paraesthesia. As the tissues rewarm severe pain is experienced with the rapid onset of a reactive hyperaemia and tissue oedema. The pain is usually transient but may become chronic with patients suffering long after tissues have recovered. Actual tissue loss is uncommon in these cases with most injuries only exhibiting mild discolouration, and very occasionally small areas of watery blisters may develop.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


