ORBITAL FRACTURES
Andrew R. Harrison, John L. Wobig, and Roger A. Dailey
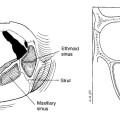
The relatively thin walls of the orbit make it susceptible to injury when orbital hydraulic forces are created by blunt trauma to the eye. Increased pressure in the orbit as a result of these injuries (e.g., a fist directly to anterior orbit) will cause the bone to “blow out” into the sinuses. The inferior and medial walls are the most susceptible to this injury. When the fracture is confined to the floor or medial wall, the term pure blow out fracture is used. With more severe injuries, the fractures can extend beyond the orbit, producing rim displacement and maxillary buttress fractures and even separating the entire midface from the skull base (Le Fort III). This chapter discusses repair of the more common orbital fractures.
Indications for blow out fracture repair of the orbital floor include rectus muscle entrapment, enophthalmos > 2 mm, and large fractures ( > 50% of the floor or wall) that will clearly lead to enophthalmos or globe malposition or both. Indications for medial wall repair are essentially the same. Generally, a 2-week waiting period is advised to clearly evaluate the need for surgery; however, in pediatric cases with clear entrapment, there is evidence that surgery should proceed as soon as possible to limit ischemic damage to the muscle. This group can also have oculocardiac reflex (bradycardia, nausea, and syncope) and this would warrant early repair.
ORBITAL FLOOR (BLOW OUT) FRACTURE
Historically, these fractures were approached through a subciliary incision or through a laceration of the lower lid sustained during the injury. Lower lid retraction and lagophthalmos were common problems following these repairs. Over the past 10 to 15 years, a transconjunctival approach to the orbital floor has gained more widespread acceptance and the incidence of complications has gone down significantly.
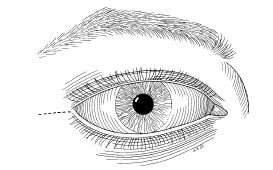
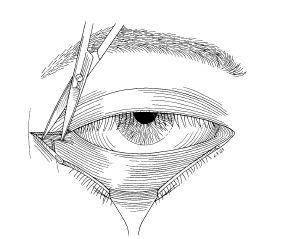
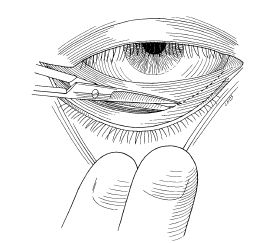
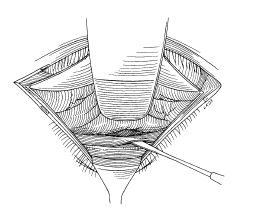
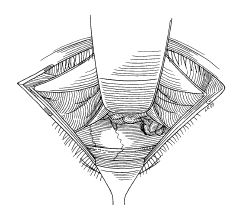
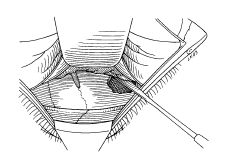
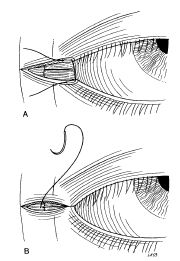
The lateral canthal and lower eyelid areas are infiltrated with 1% lidocaine with epinephrine (1:100,000) mixed 50:50 with 0.5% Marcaine(bupivacaine).Forced mine the amount of restriction prior to repair. Using a No. 15 Bard-Parker blade or CO2 laser, a 10 to 15 mm lateral canthotomy is performed in a relaxed skin tension line (crow’s foot line) (Fig. 19-1). Using a curved iris scissors, laser, or monopolar cautery, the incision is carried down to the lateral orbital rim periosteum over the zygoma. The inferior crus of the lateral canthal tendon is released (Fig. 19-2). The conjunctiva and inferior lid retractors are incised 2 mm below the tarsus from the lateral canthus incision to just lateral to the caruncle (Fig. 19-3). Having the assistant pull down on the lower eyelid skin with two fingers facilitates this incision. A Desmarres retractor is used to retract tarsal conjunctiva anteriorly and the incision is deepened to the orbital rim periosteum. The orbital septum and fat are retracted with an appropriate-sized malleable retractor. The inferior orbital rim periosteum is incised and gently dissected from the orbital floor with a Freer elevator (Fig. 19-4). The malleable retractor is repositioned in the subperiorbital plane and the fracture is exposed (Fig. 19-5). Bleeding is controlled with monopolar cautery. Herniated orbital tissue is gently elevated through the fracture site with blunt dissection until the entire rim of the fracture can be identified (Fig. 19-6). If the orbital contents are entrapped, the fracture may be enlarged with Kerrison rongeurs or Takahashi forceps to free the tissue. Bony fragments may be removed with Takahashi forceps. A paper or foil template is then cut and placed over the fracture site to adequately span the entire bony defect. An alloplastic sheet such as porous polyethelene Medpor (Porex, College Park, Georgia) is then fashioned using the template as a guide. Additional sheets may be placed for volume to achieve acceptable symmetry. Typically, the implant will stay in place behind the anterior orbital rim. A small flap may be cut into the anterior part of the alloplastic sheet and tucked into the fracture site if the implant tends to shift anteriorly. Forced ductions are performed to demonstrate free movement of the globe. The anterior periosteum is closed with a single 5-0 polyglactin 910 suture centrally to prevent anterior migration of implant(s). The inferior crus of the lateral canthal tendon is then sutured to the superior crus and then to the lateral orbital rim periosteum with 5-0 polyglactin 910 suture (Fig. 19-7). The lateral canthal angle is reformed with a 6-0 silk suture placed through the gray line of the upper and then lower eyelid. The lateral canthotomy skin incision is reapproximated with 5 0 Fast Absorbing Plain Gut suture (Ethicon, Inc., Somerville, NJ) in a running or horizontal mattress fashion (Fig. 19-8). The conjunctival incision is not closed. Antibiotic ophthalmic ointment is placed in the inferior fornix and over the lateral canthus.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


