, Madan Ethunandan2 and Tian Ee Seah3
(1)
Poole Hospital NHS Foundation Trust, Poole, Dorset, UK
(2)
Department of Oral and Maxillofacial Surgery, University Hospital Southampton NHS Trust Southampton General Hospital, Southampton, UK
(3)
Orange Aesthetics and Oral Maxillofacial Surgery, Singapore, Singapore
Subunits and Anatomical Considerations
The forehead can be divided into central, paramedian and lateral (temple) subunits (Fig. 6.1). In addition, the subunits can be further divided into upper and lower segments for the purposes of reconstruction.

Fig. 6.1
Forehead subunits
The supraorbital and supra-trochlear nerves traverse the bony orbital margins, pierce the overlying muscles and run in the subcutaneous plane, just above the frontalis/galea up to the vertex (Fig. 6.2). If attempting to preserve the sensation of the forehead, horizontal incisions and undermining should be limited to the subcutaneous plane. In case of central vertical incisions, undermining can be undertaken in the plane deep to frontalis/galea.
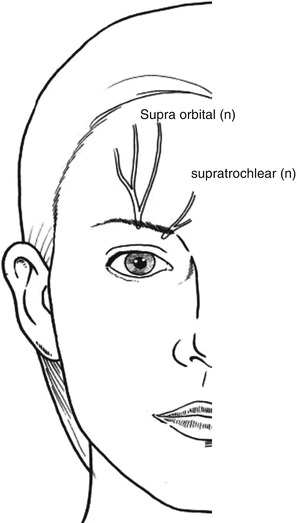
Fig. 6.2
Location of supraorbital and supratrochlear nerves
In the central forehead, the frontalis muscle is often separate in the lower part, before they join together to form a raphae. This along with the creases created by the “corrugator supercilii” offers the possibility of utilising vertical scars in this area. In the paramedian and lateral subunits, the RSTLs lie horizontally and offer good camouflage to scars (Fig. 6.3).
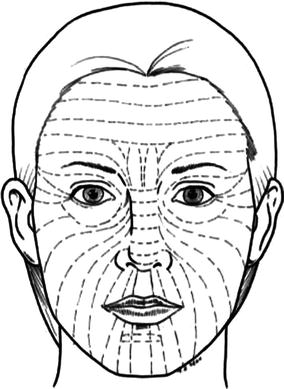
Fig. 6.3
Orientation of RSTL’s
The temporal branch of the facial nerve runs on the deep surface of the frontalis/galea and therefore incisions and dissections should be above this plane. Care should be taken to avoid distortion of the eyebrow and hairline.
Central Defects
Vertical orientation of the scars offers the best cosmetic outcome.
Elliptical Excision
Indications
Small lesion in the central subunit
Technique
The lesion is excised as an ellipse, with a vertical orientation. This enables placement of the scar along the glabellar frown lines. The margins of the defect are undermined and the wound closed in layers (Fig. 6.4a–c).
Tips
Undermining is best undertaken in the subgaleal plane to minimise damage to the adjacent sensory nerves. Consideration should therefore be given to removing additional deep tissue to facilitate dissection in the subgaleal plane. Care should be taken to accurately orient the horizontal skin creases.
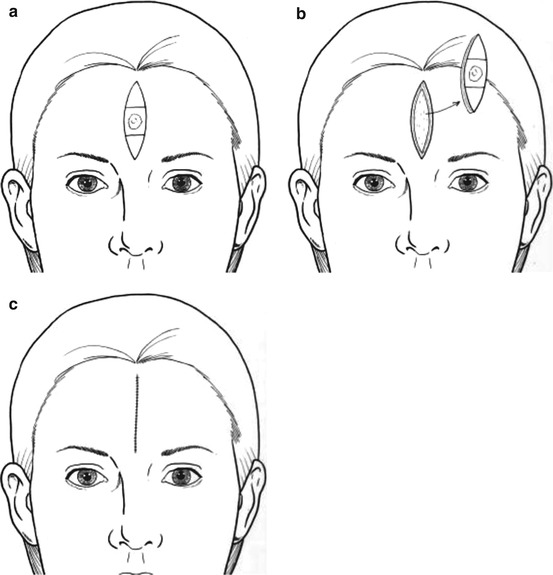
Fig. 6.4
Primary closure – Vertical ellipse
M and W Flaps
Indications
Small- and medium-sized defects in the central subunit. “W” and “M” configurations are useful for defects in the lower and upper forehead regions, respectively.
Technique
Circular defects are converted to “M” configuration and the lesion excised. The margins of the defect are undermined in the subgaleal plane and the wound closed in layers (Fig. 6.5a–c).
Tips
Undermining is best undertaken in the subgaleal plane to minimise damage to the adjacent sensory nerves. Consideration should therefore be given to removing additional deep tissue to facilitate dissection in the subgaleal plane. The “M and W” configuration decrease the overall length of the scar.
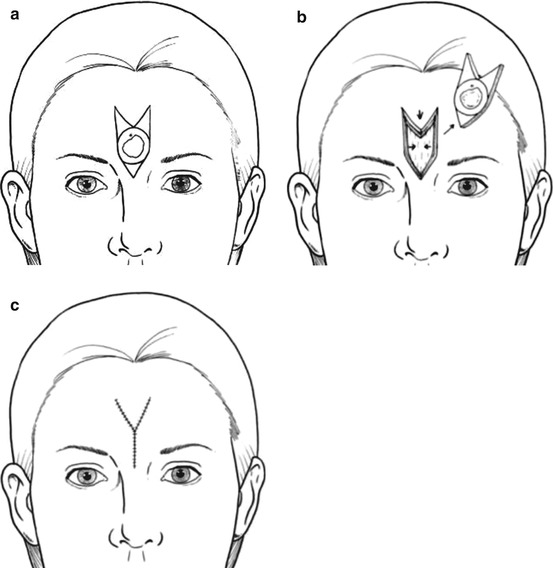
Fig. 6.5
“M” flap for central forehead defect
Upper Forehead
V-T Flap
A “V-T” flap offers the advantage of utilising a vertical scar in the central forehead and hiding the horizontal scar inside the hairline.
Indications
Medium and large defects in the upper forehead. Useful for defects that are triangular or can be converted into a triangle.
Technique
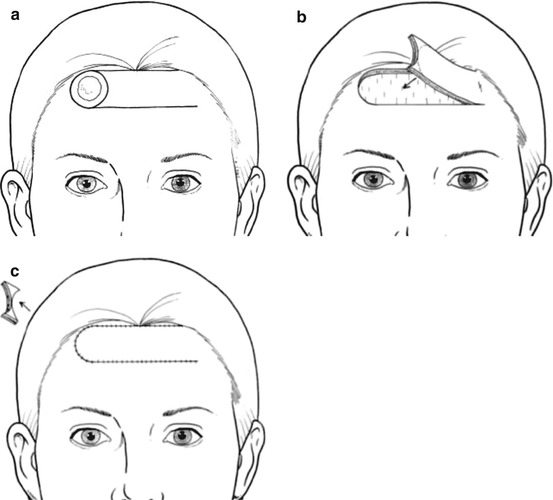
The defect is modified into a triangle. The base of the triangle is fashioned to be towards the hairline and curvilinear horizontal incisions are made laterally from the base of the defect, inside the hairline. The horizontal incisions and any undermining are best carried out in the subcutaneous plane if an attempt is made to preserve sensation to the scalp and avoid transecting the frontalis. The wound is sutured in layers and any Burow’s triangles are best positioned superiorly at the lateral margins (Fig. 6.6a–d).
Tips
Subcutaneous dissection is often tedious and is best carried out with a blade. It is essential to avoid button holing the flap and compromising the blood supply. The hairline incision is made parallel to the hair follicles to decrease the risk of alopecia. Subgaleal dissection results in a more robust flap, which is preferable for larger defects, but will result in transection of the supraorbital and supratrochlear nerve at the hairline. The difference in length of the flaps can often be accommodated by differential suturing, but if dog-ears are to be excised, these are best done superiorly inside the hairline. Care should be taken to accurately orient the horizontal skin creases.
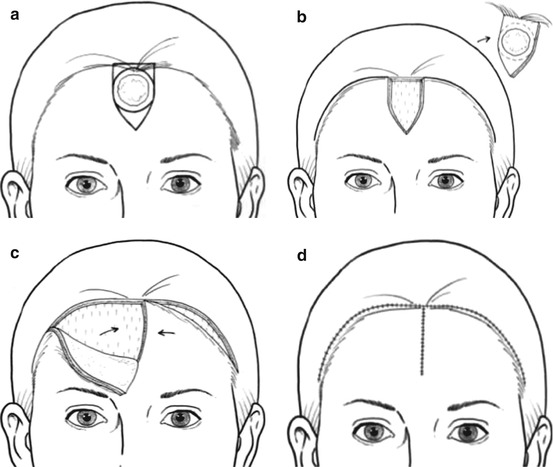
Fig. 6.6
V-T flap
Lower Forehead
A-T Flap
The “A-T” flap offers the advantage of utilising a vertical scar in the forehead and positioning the horizontal incisions along the eyebrow.
Indications
Triangular defects or defects which could be converted into a triangle in the lower forehead
Technique
The defect is converted into a triangle, with the base in the lower forehead. Horizontal incisions are extended laterally, from the base of the defect, along the forehead skin creases just above the eyebrows. The flaps are raised in the subcutaneous plane to preserve sensation to the scalp. The wound is sutured in layers (Fig. 6.7a–c).
Tips
The difference in length of the flaps can often be accommodated by differential suturing, but if dog-ears are to be excised, these are best positioned inferiorly in the glabellar region or at the lateral extremity to hide the scar in the glabellar frown lines and crow’s feet, respectively. Care should be taken to accurately orient the horizontal skin creases.
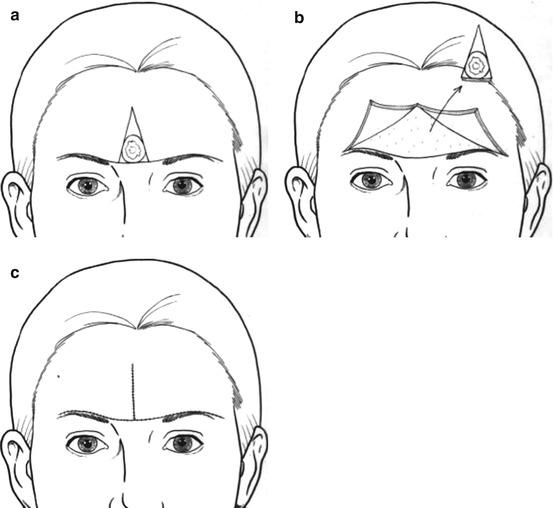
Fig. 6.7
A-T flap
Upper and Lower Forehead
Unilateral Advancement Flaps
Indications
Small and medium defects
Technique
The defect is ideally converted to obtain parallel edges. Two incisions are made from the base of the defect, parallel to each other. The margins of the defect are widely undermined and the wound sutured in layers (Fig. 6.8a–c).
Tips
In the upper forehead, one could consider expanding the defect, to place the superior incision within the hairline. The length of these incisions is ideally no more than three times the width. The flap is raised in the subcutaneous plane, if sensation is to be preserved. It is important to appreciate the difference in length (outer greater than inner) and thickness (raised flap thinner than native lateral margins) of the two flap margins and this would have to be accommodated in the suturing technique. It might be easier to place the all the sutures along the leading edge of the flap and defect margins, before tying them. If dog-ears are to be excised, these are best positioned medially in the glabellar region or at the lateral extremity to hide the scar in the glabellar frown lines and crow’s feet respectively.