Benign lesions: nevi, sebaceous hyperplasia, rhinophyma, acrochordon (skin tags), angiomas, angiofibroma, dermatofibroma, fibrous papula, keratoacanthoma, seborreheic keratosis, syringoma, venous lake, wart
Premalignant lesions: actinic keratosis
Malignant lesions: basal cell carcinoma (well-defined, small, superficial, primary, low-risk area)
Cosmetic lesions: wrinkles and laxity
Electrodesiccation
Electrodesiccation is a very common method used mostly by dermatologists, and is the process by which a mono-terminal (one treatment) high-frequency electrosurgical electrode is held in contact with the tissue, resulting in fine sparks that are absorbed by the tissue that cause thermal injury with less carbonization than that produced by electrofulguration (Fewkes et al. 1992; Chiarello 2003; Sebben 1988).
Electrodesiccation is used for very superficial lesions, such as those involving only the epidermis. The treatment electrode contacts the tissue, resulting in dehydration and coagulation. In electrosurgical destruction by electrodesiccation, when using minimal power settings, most of the damage is epidermal and there is minimal risk of scarring. However, at high power settings, there is coagulation of the deeper tissues and potential scarring. Generally, there is a combination of electrodesiccation and electrofulguration because the treatment electrode is not always in complete tissue contact and some degree of arcing occurs.
If the electrode is held at a slight distance from the tissue, a spark is formed between the electrode and the tissue—this technique, termed electrofulguration, achieves only very superficial destruction because the surface carbonization it produces insulates the underlying tissue from electrosurgical damage (Chiarello 2003; Bougthon et al. 1987). It is the method of choice when the most superficial type of tissue destruction is desired, for example, for seborrheic and actinic keratosis, spider angioma, cherry angiomas, angiokeratomas, acrochordons (skin tags), syringomata, plantar warts, condylomata, or small epidermal nevi. Hemostasis of mild capillary bleeding can also be achieved using this type of current. A standard technique for treating keratoses via this method is to move the electrode slowly across the surface of the lesion (for small lesions) or to insert it directly into the lesion (for larger lesions) while applying a current at a low power setting. After a few seconds, the lesion bubbles as the epidermis separates from the underlying dermis. It can then be removed easily with a curette or simply by rubbing a piece of gauze across the treatment site. The clinical endpoint in treating epidermal lesions is punctate bleeding, which is controlled with pressure, spot electrocoagulation, or topical hemostatic agents such as aluminum chloride. More profuse bleeding indicates probable damage to the dermis, with a greater likelihood of subsequent scarring. Extremely small superficial lesions can be treated by electrofulguration, which causes the least amount of damage to adjacent tissues (Chiarello 2003).
Electrocoagulation
Electrocoagulation is the process by which a bi-terminal high-frequency, high-current electrosurgical electrode is placed on or near tissue, resulting in significant electrical current passing through the tissue, thermally coagulating it (Fewkes et al. 1992). It is particularly useful for deep and wider tissue destruction and surgical hemostasis (clamping of a bleeding point or blood vessel). A moderately damped current is applied in a bi-terminal manner (i.e., both concentrative and dispersive electrodes are used). This current is of higher amperage and lower voltage than that utilized for electrodesiccation (Chiarello 2003; Sebben 1988). The electrode is brought into direct contact with the tissue to be treated and is moved slowly across the lesion, which eventually becomes charred. A curette is then used to remove the charred tissue.
The principal use of electrocoagulation is to obtain hemostasis of larger blood vessels. This method is indicated to treat warts, superficial telangiectases, unwanted hair, pyogenic granulomas , ingrown toenails, syringomas , xantelasma , small hemangiomas, mucous cysts, ruby angiomas , sebaceous hyperplasia , seborrheic keratoses , trichoepitheliomas , and small and uncomplicated primary basal cell carcinomas on specific areas. To treat this last condition, the procedure should be repeated two additional times in an attempt to remove any small tumor extensions. During the last curettage, a small curette is often used to remove the final tiny “roots” of the tumor. Scarring must be expected with this procedure and should be discussed with the patient (Popkin 1987; Chiarello 2003).
The user should be aware that electrocoagulation for surgical hemostasis should be applied in a dry surgical field because if there is a barrier of blood, the electrical current will be conducted through the blood and distributed over a wider area of tissue. The coagulation effect is diminished or prevented through dispersion. High power outputs should be avoided whenever possible because there will be a large mass of coagulated and carbonized tissue, which may slough and cause delayed bleeding. An alternative device for electrocoagulation is the bi-terminal forceps; both “poles” of the bi-terminal forceps are alternating active electrodes. The tissue between the two active electrodes receives very concentrated, high-current flow, and coagulation is through. Another alternative is the use of a clamp or forceps to hold the blood vessel while contact is made with the active electrode. This technique is not very useful for mono-terminal devices because the current is usually too low and too dispersed to generate sufficient heat to coagulate the vessel. However, because of its deep penetrating, destructive ability, electrocoagulation often causes inadvertent damage and necrosis of deeper adjacent tissue, which may affect wound healing and nerve function (Pollack 1991).
Electrofulguration
Electrofulguration is a process by which a mono-terminal high-frequency electrosurgical electrode is held at a distance of 3–4 mm from the tissue surface, resulting in a coarse spark that crosses the gap and causes tissue damage and carbonization.
The difference between electrofulguration and electrodesiccation is largely a matter of electrode position. The advantage of electrofulguration is that there is sufficient power to stop bleeding but less damage to the tissue than with direct contact electrodesiccation. It may also produce less scarring than electrodesiccation. High-amperage electrosurgical generators used primarily for coagulation do not produce sufficient voltage to deliver an electrofulguration current. Some units have a secondary coil added to the circuit to boost the current to a voltage level sufficient to bridge the air gap. Cutaneous lesions treated using this technique usually heal rapidly because there is very little thermal damage. The arc only needs to span a very small distance. A common error in the application of fulguration is to turn the electrosurgical machine to a very high setting so that a large visible spark arcs across a great distance. The large amount of current applied can produce excessive tissue damage, charring, and carbonization. Electrofulguration offers no advantage at high-power settings. The principal indications for using this current are solar melanose, actinic keratoses, seborrheic keratoses, and peelings (Pollack 1991).
Electrosection (Cutting)
Electrosection is a process by which a bi-terminal high-frequency, high-current electrosurgical electrode is physically passed through tissue, cutting as it goes; it is used to incise, divide, or separate tissue (Fewkes et al. 1992). Electrosection involves the bi-terminal application of a slightly damped current. The low voltage and high amperage current causes minimal lateral heat spread and tissue damage and has the additional advantage of simultaneously achieving hemostasis and cutting. “Pure” cutting can be obtained using a true undamped tube current, which provides the least amount of lateral heat spread and causes vaporization of tissue without hemostasis (Chiarello 2003). Electrosection can be used to perform rapid and effortless electrosurgical excisions or incisions without bleeding (Chiarello 2003;Sebben 1988, 1998)—virtually no manual pressure is required by the operator. Maximum power density can be achieved with a minimal amount of current; the power density value increases as the radius of the curvature on the electrode decreases. Electrosection can be performed with a variety of electrodes, the most common of which are thin wire loops. Blade-shaped electrodes are also available but tend to produce excessive thermal injury because of the greater power required and the larger surface area of the flat electrode that is in contact with the tissue as it cuts. A wire loop electrode also produces greater thermal injury than a straight-line wire electrode because of the increased electrical power required to produce the cutting power density (Fewkes et al. 1992; Sebben1998; Sebben and Davis 1988). The difference between electrosection and scalp excision is immediately apparent to the first-time user of electrosection. At the appropriate power setting, the electrode passes smoothly through the tissue like a “hot knife through butter.” However, the tissue should be hydrated continuously with wet gauze. If perceptible sparking occurs during incision, the power setting is too high; if the electrode “drags,” the power setting is too low (Chiarello 2003).
The major advantage of electrosection over scalpel surgery is that hemostasis is achieved immediately as the incision is made. However, large blood vessels (>1 mm in diameter) require additional spot electrocoagulation (Chiarello 2003) and there can be greater tissue damage and slower healing with cutting current procedures. Wounds that have been created with a cutting current can often be closed primarily, but the wound takes longer to achieve satisfactory tensile strength. Excessive energy levels or a very slow cutting speed can produce over-coagulation, a wider band of tissue damage, and poorer wound healing. Cutting should be at a steady, brisk speed. The optimum speed will cause clean separation with little or no charring—charring produces better hemostasis but causes a larger zone of thermal damage. The motion should be kept at a rate that incises the tissue adequately without a cooked or charred appearance; an optimal cutting rate of electrode movement is 5–10 mm per second (Fewkes et al. 1992; Sebben 1988, 1998). Because a small amount of charred tissue may adhere to the cutting electrode, thereby interfering with the cutting or coagulating action, the electrode should be cleaned regularly during the procedure. If char buildup seems excessive, the power may be too high or the cutting speed too slow (Fewkes et al. 1992).
Electrosurgery is extremely useful for achieving relatively bloodless excision on the head and of large bulky lesions, for incisional and shave techniques, to treat rhinophyma , hidradenitis suppurativa , and some nevus, for the excision of benign and malignant cutaneous tumors, and for skin biopsy, blepharoplasty, scalp reduction, scalp flaps, scalp lifting, and all surgical defects when allowed to heal by secondary intention (Fewkes et al. 1992; Popkin 1987; Chiarello 2003; Sebben 1988, 1998; Weber et al. 2000).
Direct-Current Surgical Galvanism
Few dermatologists have the equipment available to produce a direct galvanic current as galvanic surgery has very few useful applications in everyday practice. Its most common use is in electrolysis, a process by which low-flow direct-current electricity is passed through tissue between two electrodes, resulting in tissue damage via a chemical reaction that occurs at the tip of one of the electrodes (Fewkes et al. 1992; Sebben 1988; Sampaio and Piazza 2009). Electrolysis is commonly used to destroy hair follicles (epilation or permanent hair removal). This method is quite effective and associated with little pain and low risk of scarring, but it is a time-consuming procedure and with the laser devices available now the indication for its use is restricted to only when we want to ablate an occasional hair follicle (Shaw et al. 1988).
Electrocautery
Electrocautery uses a heat-producing electrode without the transfer of an electrical current. However, this is an old technique that is no longer in use (Sampaio and Piazza 2009). Electrodesiccation can produce essentially the same results but electrocautery can cause greater tissue damage and slower healing. High-frequency equipment has largely replaced cautery (Blankenship 1979;Sebben 1988).
Electrodes (Fig. 1)
There are different types, shapes, and sizes of electrode on the market, and they are available in a sterile or non-sterile form. The choice of electrode depends on the wave form and diagnosis of the lesion. The response by the tissue varies greatly depending on the type of electrode used. The larger the electrode, the more lateral heat produced and the higher the power setting necessary to operate it. The smaller the electrode, the less lateral heat produced and the lower the power setting necessary to operate it (Sebben 1988; Taheri et al. 2013).
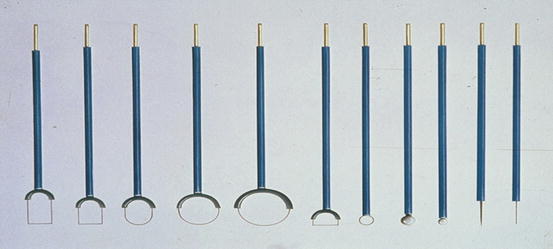
Types of Electrode
Fine needle electrode
Wire loop electrode of different sizes
Ball electrode
Desiccation-fulguration needle electrode
Wire electrode
Scalpel blade electrode
Diamond loop electrode
Ellipse electrode
Triangle electrode
Epilating needle
Bipolar forceps
Matricectomy electrode.
Fig. 1
Types of electrodes
Electrodes may be rigid or bendable. An electrode becomes less efficient as charred tissue deposits on its surface. As this occurs, the delivery of the electrosurgical current becomes less precise and higher power settings are required. Therefore, it is important to keep electrode tips clean during the course of electrosurgical procedures.
Factors Causing Less Collateral Heat Damage
Smaller electrode diameter
Shorter contact time between the electrode and lesion
Lower intensity of power
Higher frequency of current
Cutting waveform.
Electrosurgical Procedures
There are many electrosurgical devices available, and each provides a variety of waveforms—any of these machines can be used. We use the Wavetronic 5000 Digital (Fig. 2) radio-frequency device (Loktal Medical Electronics, Brazil).










