5 Following the Pattern: Hair Restoration
Summary
Hair loss can affect men of all ages, and presents in a variety of patterns. Fortunately, most men respond well to treatment with either medical or surgical treatment. Preferably, patients undergoing a hair transplant procedure will combine it with medical therapy to prevent ongoing loss and potentially enhance the results of their surgery.
Keywords: androgenetic alopecia male pattern hair loss minoxidil finasteride low-level light therapy platelet-rich plasma hair transplant surgery hair restoration
5.1 Background
The successful treatment of hair loss can improve a man’s confidence, relationships, and overall quality of life. It can also increase a man’s desire to improve other aspects of his life. He may start dating again, lose weight, or find a better job, all of which contribute to an improved sense of self-worth. When it comes to hair restoration, it is important for men to understand that they have several options spanning from noninvasive medical treatments to more involved procedures: they may choose to start slowly with medical therapy, first trying to achieve maximum growth after 1 to 5 years, or move quickly toward hair transplantation alone or, preferably, in combination with medicine. Cosmetic options like camouflage products or scalp micropigmentation (SMP) can help give them “instant” results in the short term.
5.2 Diagnosis
Male pattern hair loss presents in a wide array of clinical settings. Onset may begin as early as the teenage years, as shown in Fig. 5.1, which depicts a young man who was just 16 years when he started to develop thinning in the vertex. Some men may start to notice hair loss as they are heading off to college, presenting as early thinning or recession in the frontal hairline (Fig. 5.2). Others may not necessarily “see” hair thinning; instead, they may just complain of more hair on their pillow or in their hands when they shower.

Fig. 5.1 Vertex thinning in a 16-year-old adolescent boy.

Fig. 5.2 Frontal thinning in a 19-year-old man.
It is important for clinicians to try to be both compassionate and aggressive in offering treatment to these young men. Do not exclude male pattern hair loss from the differential diagnosis simply due to the patient’s young age. With every patient, ask carefully about a family history of hair loss. Be sure to include female relatives in the discussion. Patients may be quick to deny any family history of hair loss, but often forget about the opposite gendered parent or other genetically related individuals.
For men, the Hamilton-Norwood system is used to grade the degree of hair loss. It accounts for the different patterns of hair loss, which can start with isolated thinning in the vertex, recession of the frontal bitemporal hairline, or in a diffuse unpatterned alopecia (DUPA) that mimics female pattern hair loss (Fig. 5.3).

Fig. 5.3 Diffuse unpatterned alopecia (DUPA) in a 30-year-old man.
Dermoscopy can be an excellent guide in diagnosing male pattern hair loss. The presence of miniaturized hairs along the frontal aspect of a receding hairline or in a thinning vertex can help confirm the diagnosis, especially if the patient also has a family history of hair loss. It is helpful to explain to patients that this miniaturization process is inherited, as thick terminal hairs are replaced by miniaturized versions of themselves over time (Fig. 5.4). Not only are the new hairs coming in finer and thinner, but they are also growing for a shorter period of time. The anagen, or growth, phase can shorten from 5 to 7 years to 3 to 4 years to 1 to 2 years, and as a result of these shorter cycling times, the hairs will appear to fall out more quickly.

Fig. 5.4 Miniaturized hairs as seen on dermoscopy.
5.3 Mimickers of Male Pattern Hair Loss
Occasionally, patients may present with diffuse shedding. This can be the result of telogen effluvium, a temporary shedding often due to a major physiologic or psychologic stressor, or a lab abnormality. Obtaining labwork is recommended for these patients, especially if they have no known family history of hair loss. The most common laboratory abnormalities associated with new-onset hair shedding are observed with thyroid, zinc, iron, and vitamin D.1 Patients taking Accutane or high-dose vitamin A supplementation may present with temporary hair shedding. Diffuse alopecia areata can also present with diffuse shedding, as in the gentleman depicted in Fig. 5.5 who quickly experienced hair regrowth with oral prednisone and topical steroid shampoo.
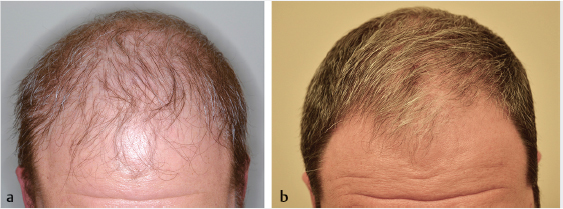
Fig. 5.5 (a) A male patient with diffuse alopecia areata, before treatment. (b) A male patient with complete regrowth of alopecia areata, after treatment.
Patients may complain of scalp symptoms like itching, burning, or tenderness in the context of hair loss. This should expand the clinician’s differential beyond pattern hair loss. In these cases, obtain a complete history of when the symptoms began and what therapies they have tried (over-the-counter or prescription) and which helped. Such symptoms may point the clinician toward other mimickers of male pattern hair loss, such as frontal fibrosing alopecia (FFA) or lichen planopilaris (LPP), two types of cicatricial alopecia. The patient in Fig. 5.6 presented with long-standing, asymmetrical frontal hairline recession and also had loss of eyebrows and sideburns to support a diagnosis of FFA. These inflammatory causes of hair loss must first be addressed using topical steroids, oral doxycycline, and/or hydroxychloroquine. Hair transplantation may be possible on a case-to-case basis, but only after the disease process has been stabilized.

Fig. 5.6 Top view of a 67-year-old man with frontal fibrosing alopecia (FFA) demonstrating asymmetric hair loss.
During initial consultation, it is helpful to explain to men that the two main approaches available to achieve hair regrowth are nonsurgical and surgical. Nonsurgical therapy includes medications that affect molecular signaling to stimulate the thinner, finer, hairs to cycle back as thicker, fuller versions of themselves. This approach will not only help stabilize ongoing hair loss but will also help slowly regrow hair starting as early as 6 months. By combining medical therapies, synergistic results can be achieved with maximum regrowth over 3 to 5 years.
5.4.1 Nonsurgical Options for Hair Loss
There are two Food and Drug Administration (FDA) approved medical therapies available to patients: oral finasteride and topical 5% minoxidil solution and foam (Fig. 5.7). It is important to present these options first, as they exhibit the most robust data to support their use and are generally well tolerated. Other off-label therapies for hair loss include oral dutasteride, topical finasteride, oral minoxidil, low-level light therapy (LLLT), and platelet-rich plasma (PRP). A number of supplements as well as plant-based 5-alpha reductase inhibitors such as saw palmetto and pumpkin seed oil are also currently available.

Fig. 5.7 Oral finasteride and topical minoxidil are Food and Drug Administration (FDA) approved treatments for male pattern hair loss (MPHL).
5.4.2 FDA-Approved Nonsurgical Options
Topical minoxidil was approved in the 1980s under the trade name Rogaine. It was initially studied as an oral antihypertensive medication, but was found to have the unwanted side effect of hypertrichosis. Johnson & Johnson subsequently conducted randomized clinical trials for a 5% solution that was ultimately approved for twice daily application in men. Now the foam vehicle is also FDA approved for twice daily application.
Minoxidil can be very effective, but as with any medical therapy, patients must be compliant for 4 to 6 months before they will start noticing results (Fig. 5.8). Patients are encouraged to use it in an open-ended fashion, just as they would brush their teeth. Although rare, patients may develop an allergy to minoxidil, and should also be informed that the solution formulation contains the preservative propylene glycol, which is a known contact allergen.2 Patients who report itching with the solution should switch to the foam before discontinuation of all topical minoxidil.
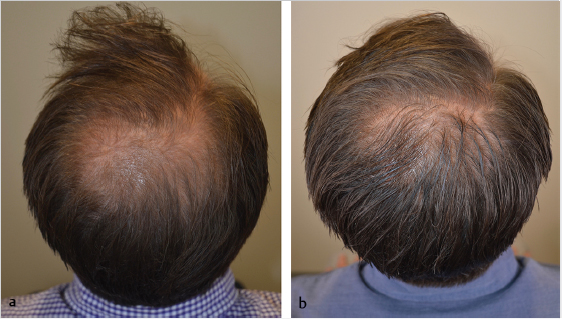
Fig. 5.8 (a) Vertex view of a 41-year-old man before treatment with topical 5% minoxidil. (b) Vertex view of the same patient 6 months after treatment with topical 5% minoxidil.
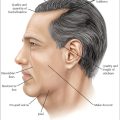
Oral finasteride became FDA approved in 1992 under the trade name Proscar at a 5-mg dose for benign prostatic hypertrophy (BPH). When it was observed that patients on this medication were experiencing hair regrowth, researchers began studying oral finasteride for its hair regenerative properties. Clinical trials demonstrated that a 1-mg daily dose was sufficient to help regrow hair. Whereas these trials evaluated the vertex scalp, this area was selected specifically for ease of standardization and imaging. Oral finasteride has since been shown to successfully grow hair in the frontal scalp as well (Fig. 5.9).3
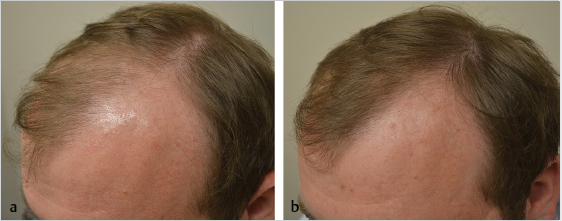
Fig. 5.9 (a) Side view of a 35-year-old man before treatment with oral finasteride 1 mg daily. (b) Side view of the same patient 6 months after treatment with oral finasteride 1 mg daily.
In 1997, the medication was approved by the FDA for hair loss, under the trade name Propecia. Finasteride works by blocking the conversion of testosterone to dihydrotestosterone (DHT), via type 2 5-alpha reductase. Some men worry that this treatment may cause unwanted facial hair or body hair growth. However, because the type 2 5-alpha reductase enzyme only exists in the scalp and the prostate, this is of little concern. As long as vellus hairs are intact on the scalp, darkening and thickening of such hair is possible. However, where hairs have fully involuted and the scalp appears shiny, there may be less opportunity for regrowth.
In a study from Japan, finasteride was found to be 80 to 90% effective for men in every decade of life.4 We know from clinical trials that the degree of regrowth that can be achieved generally plateaus by around the fifth year of use. The drug can be taken either as a 1-mg pill or as one-fourth of a 5-mg pill daily. The latter option is generally less expensive but may result in less accurate dosing, depending on how well the patients are able to quarter the pill and how evenly the drug is distributed within the pill. Patients with BPH may benefit from the full 5-mg pill daily.
Finasteride can be taken with or without food, any time of day, and has not been reported to cause any allergies or known drug interactions. If patients are otherwise well with normal liver function tests, no laboratory monitoring is required. It is permissible for a man to start a family while he is taking finasteride. However, men who are taking finasteride are not permitted to donate blood due to the possibility of birth defects among pregnant women who are potential recipients. For the same reason, women of childbearing potential should not take or touch the drug. Taking finasteride can artificially lower a man’s prostate-specific antigen (PSA) and interpreting physicians should double the PSA in order to obtain the true value.5
Controversy exists regarding whether finasteride may cause long-term sexual side effects even after discontinuation of the medication.6 Many studies have been limited by selection bias, recall bias, or lack of control for confounding variables—specifically causes of erectile dysfunction such as vascular disease, diabetes, depression, and smoking.7 The term post-finasteride syndrome (PFS) has been used to describe a constellation of symptoms including depression and brain fog. As mentioned earlier, although it has not yet been determined that finasteride is the cause of such outcomes, the manufacturer has altered their packaging to reflect this possibility. Some hair loss specialists screen patients for preexisting anxiety, depression, or panic attacks with the concern that they may be at higher risk of developing PFS.
5.4.3 Off-Label Nonsurgical Options
Oral minoxidil has been used more recently as an alternative to the topical formulation as a means to improve compliance. When dosed as 10 or 20 mg under the trade name Loniten, it has been associated with a number of side effects including peripheral fluid retention and pericardial effusion. However, at lower doses of 0.1 to 0.625 mg (one-fourth of a 2.5-mg tablet), it can be helpful and well tolerated. Patients who are interested in the oral medication may want to first consult with their primary physicians, especially if they are already on other blood pressure–lowering agents. It is not FDA approved in this formulation for hair loss.
Dutasteride is a sister drug to finasteride, approved only for BPH. It blocks both type 2 and type 1 5-alpha reductase, making it theoretically even more effective than finasteride. However, it has a much longer half-life, lasting 170 to 300 hours in the body. As a result, the potential side effects of libido change or a reduction in sperm count may last for a much longer time. For this reason, it is not recommended for use in young men who may want to conceive and would not want the potential long-term effects of sperm reduction. It is still only FDA approved for hair loss in Korea.
Dutasteride has been used in combination with finasteride for men who have achieved a plateau in terms of hair regrowth. One published protocol that resulted in additional regrowth in the vertex scalp suggests a loading dose of 0.5 mg daily for 2 weeks, followed by weekly dosing in combination with 1-mg oral finasteride.8 Other patients who suffer from BPH may consider going straight to dutasteride 0.5 mg daily and insurance may cover their drug cost.
LLLT involves the delivery of 600- to 700-nm infrared light via a hairbrush, headband, cap, or helmet. Many devices are now commercially available and some have received 510(k) FDA clearance as devices. They vary in their instructions for usage but generally require three to five treatments weekly, lasting 20 to 30 minutes each. The treatments are safe with no known side effects. The cost of these devices varies from $300 to $3,000, based on the number of diodes and intensity of light emitted. Unfortunately, we do not yet have any head-to-head studies showing the most effective device, but they all generally seem to have the same mechanism of action.
PRP has gained a lot of attention for its role in dental and orthopaedic medicine, specifically related to wound healing and in joints. More recently, dermatologists have investigated its ability to upregulate hair follicle growth and there is an increasing amount of basic science data to support this application. To obtain a sample of PRP for injection, venous blood is first collected from the patient and then spun down using a high-speed centrifuge to separate off the golden platelet-rich portion. Alpha granules within the platelets contain growth factors such as platelet-derived growth factor (PDGF), epidermal growth factor, and vascular endothelial growth factor (VEGF). The proposed hypothesis for PRP’s effects is that when injected as aliquots of 0.1 to 0.5 mL over areas of hair thinning, plasma containing these growth factors can help enhance growth of hair follicles. Various protocols have been described in the medical literature, using the PRP alone, or adding various “activators” such a calcium gluconate or calcium chloride. A large number of commercially available PRP preparation kits are available.
Many questions remain with regard to the optimal protocol for PRP. What matters most: the concentration or absolute number of platelets injected? One recent publication demonstrated increased hair growth irrespective of platelet counts or quantification of growth factors.9 How often should the PRP be administered? Does it need to be activated with exogenous agents such as calcium chloride or can the platelets become activated as a result of simple contact with collagen? What is the role of other additives such as matrices and can these products further improve PRP’s efficacy?
Topical finasteride has been investigated as a means of delivering 5-alpha reductase blockade without the development of sexual side effects. One recent meta-analysis suggested that a 0.25% concentration could successfully lower scalp DHT levels without affecting serum DHT levels.10 One possible setback is that this product must be formulated by a compound pharmacy; however, this can provide the opportunity to combine it with topical minoxidil for synergistic results. In addition to finasteride, there is also evidence that topical tretinoin may help enhance the efficacy of topical minoxidil.11
Many over-the-counter supplements are available for hair regrowth. Viviscal Pro contains the proprietary AminoMar complex containing marine proteins such as shark cartilage and oyster shell, as well as procyanidins, which have antioxidant effects.12 Nutrafol is another commercially available hair supplement that contains newer antioxidant ingredients like ashwagandha and a proprietary biocurcumin.13 Supplements advertised for prostate health contain the plant-based 5-alpha reductase inhibitors saw palmetto and pumpkin seed oil, which have some limited data to support their use.14,15 Biotin is frequently used for hair loss but has no data to support its use for androgenetic alopecia.
5.5 Choice of Nonsurgical Therapy
Clinicians must carefully watch for verbal and nonverbal cues during the initial consultation with a male hair loss patient. Some men will express little to no interest whatsoever in medical therapy, either as a result of previous treatment failure, perceived inefficacy, or concerns about side effects. These men may be more amenable to other nonsurgical treatments such as LLLT or PRP, or they may directly express a preference for surgical options as definitive treatment. Still others may be excellent surgical candidates but are not prepared to pursue hair transplantation.
It is incumbent upon the surgeon to explain the risks, benefits, and alternatives—including no treatment—of the various treatment options for male pattern hair loss. Additionally, it is important to discuss and establish realistic expectations. As an example, the authors use the analogy of male pattern hair loss as a leaky bathtub. The patient presents for treatment because they are unhappy with the level of water in the tub. Hair transplantation moves hair from the back of the scalp to the front—like pouring a big bucket of water into the tub. Patients get a nice one-time rise in the level of water in the tub, but surgery alone does nothing to prevent ongoing hair thinning. It is helpful to explain that utilizing one or more nonsurgical medical therapies is the equivalent of plugging the leak in the bottom of the tub. Patients must understand it does not matter what type of medical therapy they use, just that they consider something to help stop the ongoing hair thinning.
5.6 Surgical Options for Hair Loss
Hair transplantation has evolved considerably over the years. In 1939, Dr. Shoji Okuda of Japan was one of the first to use punch grafts to treat hair loss due to alopecia areata, leprosy, and cicatricial alopecia. In 1959, Dr. Norman Orentreich began using punch grafts at NYU, ultimately establishing a successful private hair transplant practice in Manhattan.16 Although the initial surgical transplantation of hair loss was a surgical success, it was considered a cosmetic failure by many based on the “plug” appearance of these punch grafts. Terms like “picket fence” and “doll hairs” evolved to describe the unnatural appearance of many of these early transplants.
Dr. O’Tar Norwood, a dermatologist from Oklahoma, worked tirelessly to advance the field of hair surgery. In 1990, he compiled the first Hair Transplant Forum publication. In 1993, Dr. Norwood, Dr. Dow Stough, and others founded the International Society of Hair Restoration Surgery, organizing the first and largest meeting devoted strictly to hair and scalp surgery. It was held in Dallas, and there were 430 attendees, 80 assistants. Since that time, the society has grown to over 1,100 members representing 70 countries worldwide.
In 1994, Dr. Bobby Limmer suggested the use of stereoscopic microscopes to separate the hairs into their native follicular groupings of one to four hairs each (Fig. 5.10).17 He modernized hair surgery by making the hair look more natural and better able to mimic the appearance of surrounding hairs. He also paid close attention to matching the existing hair angle in order to avoid placing hairs too perpendicularly, or in the vertex scalp where continued loss could result in an unnatural-looking island of transplanted hair.
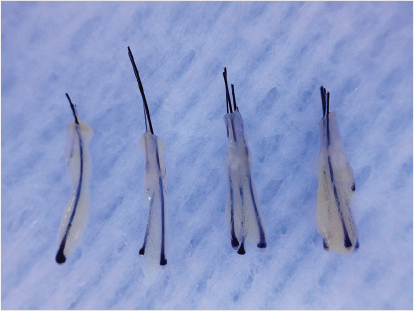
Fig. 5.10 Microscopic image of scalp demonstrating one- to four-hair follicular units.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


