CHAPTER 7 Femoral Osteotomy
Proximal femoral osteotomies belong to the category of so-called hip joint–preserving surgeries, which are defined as surgical treatments of prearthritic hip deformities or of early hip osteoarthritis which maintains the biologic joint. Although proximal femoral osteotomies are constantly decreasing in number, there are good indications for these procedures. Valgus-type osteotomies are indicated in post-traumatic deformities and nonunions near the hip, flexion/extension osteotomies in hips with avascular necrosis, and varus-type osteotomies for dysplasia.1–4 This chapter describes the detailed surgical technique of intertrochanteric osteotomy (ITO) without removal of a wedge; its indications and perioperative management; and tips, pearls, and current concepts in joint-preserving hip surgery.
INDICATIONS AND CONTRAINDICATIONS
Theoretically, ITO provides correction of the femoral axis in the frontal, the sagittal, or the transverse plane with or without leg length shortening.1,3 Historically, the basic rationale for ITO was to reduce or improve the distribution of forces loading the hip, and numerous indications led surgeons to perform this procedure (Table 7-1). Nevertheless, total hip arthroplasty has supplanted ITO for several reasons, including difficult definition of the indications, the demanding nature of the intraoperative technique for ITO, and the unpredictability of its results. Presently, ITO should be considered only when the correction provides improvement in coverage, containment of a normal head portion, leg alignment, or congruency.
TABLE 7-1 INDICATIONS FOR DIFFERENT TYPES OF INTERTROCHANTERIC OSTEOTOMIES
| Frontal Plane | |
| Valgus osteotomy | Femoral neck pseudarthrosis |
| Marked post-traumatic varus deformities | |
| Circumscribed anterolateral necrosis of the femoral head or epiphyseal dysplasia with intact medial part of head | |
| Equivalent of improved hip joint congruency on functional radiographs (or fluoroscopy) in adduction, in particular when accompanied by an adduction contracture | |
| ≥15 degrees of passive adduction with pain relieved in adduction (with or without flexion) | |
| Varus osteotomy | Marked coxa valga with a neck-shaft angle >140-150 degrees |
| Valgus head, in particular when the fovea lies in the weight-bearing zone of the acetabulum | |
| Circumscribed anteromedial necrosis of the femoral head or epiphyseal dysplasia with intact lateral part of head | |
| Equivalent of improved hip joint congruency on functional radiographs (or fluoroscopy) abduction, in particular when accompanied by an abduction contracture | |
| Developmental hip dysplasia with concomitant malposition in valgus of the proximal femur, on the condition that a pelvic osteotomy cannot sufficiently restore the femoral coverage | |
| ≥15 degrees of passive abduction with pain relieved in abduction (with or without flexion) | |
| Osteochondrosis dissecans | |
| Sagittal Plane | |
| Flexion osteotomy | In combination with valgus/varus intertrochanteric osteotomy to rotate altered segments out of the weight-bearing zone |
| Slipped capital femoral epiphysis with excessive posterior tilt of the femoral head | |
| Extension osteotomy | Fixed flexion contracture (rare) |
| Transversal Plane | |
| Rotational osteotomy | In combination with varus osteotomy, eventually acetabuloplasty, persisting marked coxa valga with anteversion exceeding the normal age-related angle of anteversion by 20 degrees |
Intertrochanteric flexion or extension osteotomy for osteonecrosis has declined in popularity because of its questionable long-term results. This procedure may still be used for treatment of early-stage necrosis, however, with a circumscribed segmental extension of the lesion. A second indication for flexion/abduction osteotomy may be a slipped capital femoral epiphysis with an excessive posterior tilt of the femoral head. Table 7-2 lists absolute and relative contraindications for ITO.
TABLE 7-2 ABSOLUTE AND RELATIVE CONTRAINDICATIONS FOR INTERTROCHANTERIC OSTEOTOMY
| Absolute Contraindications |
| Severe osteoporosis |
| Advanced osteoarthritis with marginal osteophytes |
| Marked spasticity or excessively stiff hip |
| Inflammatory arthritis |
| Joint incongruency, made worse with adduction if valgus osteotomy or with abduction if varus osteotomy is planned |
| Relative Contraindications |
| Obesity (body mass index >30) |
| Age >60 years |
| Cigarette smoking |
PREOPERATIVE PLANNING
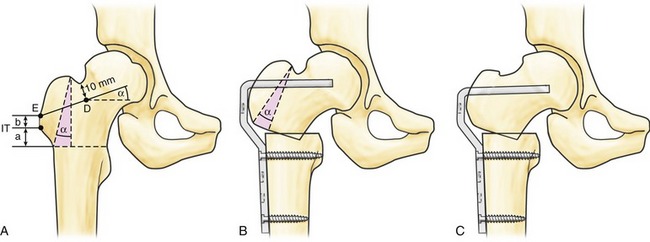
A varus osteotomy is planned as follows (Fig. 7-1).
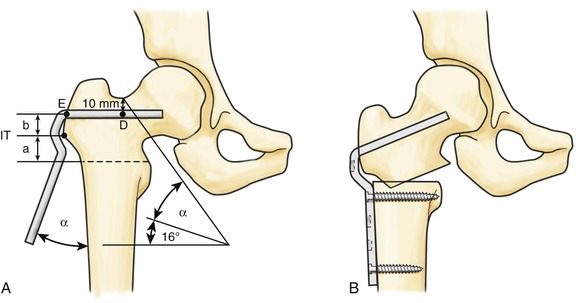
The first planning step of a valgus osteotomy starts with the determination of the correction angle (Fig. 7-2). In case of a femoral neck pseudarthrosis, the aim is to convert shear stresses into compressive forces, increasing the likelihood of union. The amount of valgization can be determined by subtracting 16 degrees (which represents the normal compression vector force on the hip [Fig. 7-3]) from the Pauwel angle (defined as the angle between the pseudarthrosis and a horizontal line). Next, the site of osteotomy, the innominate tubercle, the distance a, and point D are determined. The virtual blade is overlaid on the anteroposterior radiograph by constructing the planned valgus alpha angle relative to the femoral axis and by caudocranial translation through point D. The distance a between the innominate tubercle and the entry point E of the blade can be used as an intraoperative reference.