CHAPTER 40 Femoral Component Removal













TECHNIQUE
Tools and Specialized Equipment
Ultrasonic tools are sometimes useful for removing cement from the intramedullary femoral canal.1 Specially designed tool tips convert electrical energy to mechanical energy that is concentrated at the cement mantle, thereby breaking it down. When cortical bone is contacted instead of cement, auditory and tactile feedback can prevent canal perforation.2,3 Because more force is required to break cortical bone than cement, the ultrasonic system is generally safe, and this has been validated clinically.4 Limitations include a learning curve and the expense of purchasing or renting the ultrasonic equipment. If the equipment is not available, alternatives to removing retained cement in the femoral canal include the use of hand tools, facilitated by an extended osteotomy of the femoral canal that can expose the entire cement mantle.
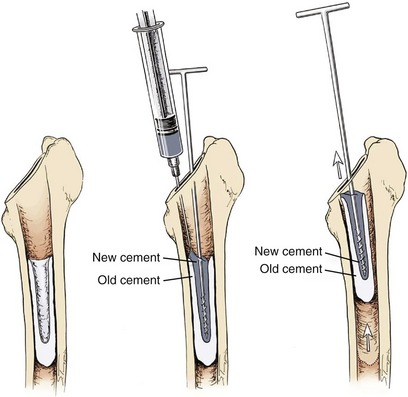
In some revision procedures the existing cement mantle may have separated from the femoral cortices and fragmented into loose pieces. In such situations, one removal strategy is to introduce new cement into the femoral canal that can bond to the old cement and remove it in 1- to 2-cm–long segments with an extraction rod anchored in the new cement mantle (Fig. 40-1). If indicated, this strategy requires the availability of special equipment (SEG-CES, Zimmer, Warsaw, IN).
Extraction tools that can help pull the femoral implant out of the canal include modular femoral head and neck detachment devices and femoral stem extractors. Universal femoral extractors for modular and nonmodular components and special extractors that insert into a hole in the prosthesis or fit tightly around the prosthetic femoral neck can greatly facilitate implant removal and save operative time. In addition to extractors, a set of long-handled bone punches with and without offset built into the instrument should be available to impact the stem against the collar (if any) and assist in stem extraction (Fig. 40-2).







