CHAPTER 37 Extended Trochanteric Osteotomy
Posterior Approach
KEY POINTS
 Consider an extended trochanteric osteotomy for the removal of well-fixed implants, for the removal of retained distal cement, and for patients demonstrating varus femoral remodeling.
Consider an extended trochanteric osteotomy for the removal of well-fixed implants, for the removal of retained distal cement, and for patients demonstrating varus femoral remodeling.



INDICATIONS
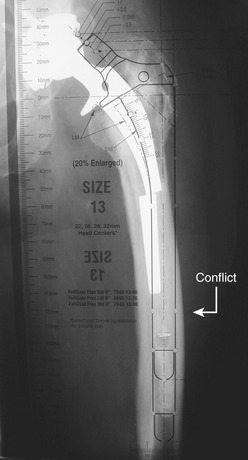
The most common indications for the use of an extended trochanteric osteotomy include removal of a well-fixed femoral implant; removal of retained distal cement; insertion of a femoral component in patients with proximal femoral remodeling; and improved surgical exposure (Fig. 37-1).