Examining the skin
The skin needs to be examined in good, preferably natural, light. The whole of the skin should be examined, ideally; this is essential for atypical or widespread eruptions (Fig. 1). Looking at the whole skin often reveals diagnostic lesions that the patient is unaware of or may think unimportant. In the elderly, thorough skin examination often allows the early detection of unexpected but treatable skin cancers.
 note the distribution and colour of the lesions
note the distribution and colour of the lesions


 wear gloves when examining the mouth, genitals and perineum or if lesions may be infected
wear gloves when examining the mouth, genitals and perineum or if lesions may be infected

Distribution of eruption or lesions
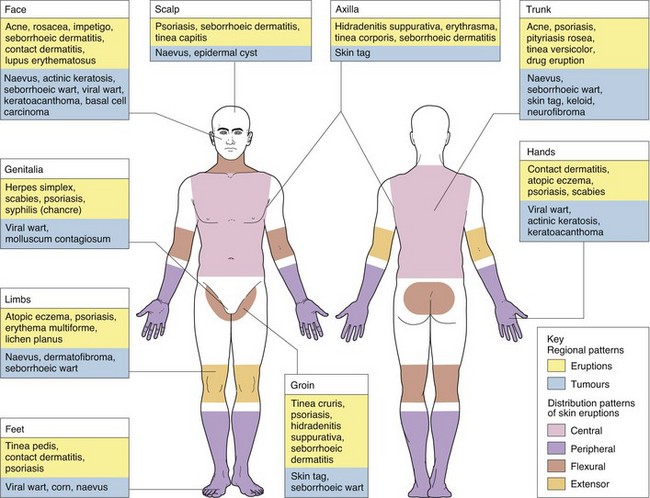
Stand back from the patient and observe the pattern of the eruption (Fig. 1). Determine whether it is localized (e.g. a tumour) or widespread (e.g. a rash). If the latter, determine whether the eruption is symmetrical and, if so, peripheral or central. Note whether it involves the flexures (e.g. atopic eczema) or the extensor aspects (e.g. psoriasis). Is it limited to sun-exposed areas? Is it linear?
Dermatomal patterns are also seen. Herpes zoster (shingles) is the commonest example of this, but some naevi also appear in this guise or follow Blaschko’s lines (p. 13). Regional patterns (see Fig. 1), e.g. involvement of the groin or axilla, will suggest certain diagnoses to the experienced physician. For example, guttate psoriasis and tinea versicolor tend to occur on the trunk, whereas lichen planus often occurs around the wrists, and contact dermatitis frequently affects the face, feet or hands. The factors resulting in these patterns are complex but include skin anatomy, e.g. blood vessels, nerves, appendages or embryonic lines, and environment, e.g. moist conditions in the axillae, chemical contacts and sun exposure.



