6
Endoscopic Forehead Lifting
Gregory S. Keller, P. Daniel Knott, and Robert W. Hutcherson
The brow is the most important feature of the upper third of the face, representing the central facial aesthetic signature when considered in concert with the eyes and nose. The human eye is naturally drawn to this central triangle, and subtle differences in the representative sizes, shapes, and shadows of its constituent parts are immediately translated into a perception of beauty and a sense of overall chronological age.1 Facial features distant from this core triangle carry a disproportionately lesser weight in the consideration of overall age and beauty. A thorough evaluation of ideal brow position must therefore figure prominently in any successful overall rejuvenative intervention.
The movement of the brows and the furrows created by the various brow elevators and depressors are extremely important components in facial expressivity. Whether rising with surprise, converging with uncertainty, or descending with anger, the brows translate emotion into expression. Whereas this emotional expressivity is manifest by constant change in brow position in the short term, in the long term such change becomes static. In fact, an individual’s predominant expressions become steadily ingrained in the upper third of the face over time, much as a cliff face becomes chiseled over the years by the combined influences of wind and rain. Brow position and the surrounding periorbital rhytides therefore reveal the expressive muscular actions that have been etched over time. The goal of effective brow rejuvenation incorporates an understanding of these cumulative emotive influences, aiming for the establishment of a softer, more pleasing and youthful curve and shape.
♦ Brow Analysis
The position of the brows at rest necessarily represents equilibrium between the forces of agonism and antagonism.2 The corrugator supercilii, procerus, depressor supercilii, and orbicularis oculi are the agonist muscles, which lower and corrugate the brow. The frontalis muscle is the sole antagonist that raises the brow. Gravity exerts the most important exogenous influence, inexorably leading to the stretching of the periorbital soft tissues and the loss of the resting tone of the frontalis muscle. This leads to descent of the brows in relation to the fixed point of the supraorbital rim. The effort to balance this descent leads to frontalis muscle overactivity and the creation of horizontal forehead rhytides. The process of progressive brow ptosis occurs more markedly at the lateral brow, producing lateral canthal hooding and brow overhang. Any consideration for manipulation of brow position must at its inception incorporate a cogent overall strategy encompassing eyelid function and position. The position of the brows, via attachments of the arcus marginalis to the supraorbital rim and via the septum to the tarsus and upper eyelid skin, has a defined relationship to upper lid position. Although this chapter will not focus on upper lid position, a clear understanding of these relationships must precede any operative intervention.
Aesthetic interpretation of the brow does not follow absolute standards, and surgical goals must be based on what appears correct for a given patient. Cultural, structural, gender, and age issues are factored in when preoperative goals are being planned. However, forehead aesthetic considerations can draw on quantifiable guidelines. Leonardo da Vinci outlined facial proportions with his rule of vertical thirds and horizontal fifths. In the rule of thirds, the distance from hairline to the bottom of the high point of the brow should equal the distance from the inferior brow to the nasal base, which in turn should equal the distance from the nasal base to the bottom of the chin. In the rule of fifths, the face is divided vertically into five equal columns whose width equals that of the eyelid (see Chapter 2). The eyebrow should approximate or be slightly above the superior orbital rim, and the apex of the arch should be at a point tangent to the lateral limbus, or approximately two thirds of the way from the medial brow to the brow tail. The tail of the brow should be on an oblique line from the lateral alar rim through the lateral canthus. The medial brow margin is tangent to a vertical line drawn from the lateral ala through the medial canthus. The medial and lateral brow should be in the same horizontal plane. Racial differences are often subtle, but notable. In the Asian, Latino, and African-American populations, an aesthetically pleasing origin to the medial brow is tangent to a line bisecting the nasal lobule and the medial canthus. Gender differences must also be distinguished. Female patients have a forehead height aesthetic of 4 to 6.2 cm (average 4.8 cm), whereas male forehead height typically ranges from 6 to 7 cm. Women have a smoother forehead contour from the supraorbital rim to the hairline. Men have a more prominent lateral supraorbital rim with a tendency to frontal bossing.
Preoperative analysis and planning are critical to creating the desired surgical outcome for any procedure. In brow lift surgery, defining the goals of the surgeon and setting appropriate expectations for the patient are important parts of the operative strategy. Incorporating the visual and quantitative criteria noted above will help achieve these goals. Indications for foreheadplasty surgery are brow ptosis, glabellar ptosis, and vertical glabellar furrows. Assessment of the patient should focus on frontal hairline contour, hair density, and brow contour. Attempts have been made to objectify the analysis of brow position to optimize outcomes of endoscopic foreheadplasty. McKinney et al brought forth the concept of frame height, which is the distance from midpupil to the top of the brow.3 Under this definition, brow ptosis exists if this distance is less than 2.0 to 2.5 cm, and a brow lift procedure is indicated. Sasaki combined the concept of frame height with the concept of brow mobility, using a “glide test” to predict the effectiveness of endoscopic brow lifting procedures.4 The glide test is a measurement of maximal brow excursion in the medial, central, and lateral vectors under manual pressure from the examiner. Optimal results after endoscopic brow lifting were obtained when the frame height was 1.5 to 2.0 cm and the glide test values were 2 to 3 cm. These parameters are consistent with a ptotic brow with significant forehead laxity. A standard facial photographic series should be obtained.
♦ Anatomic Considerations
Brow Elevators
The principle brow elevator is the frontalis muscle. With its origin at the skin and superficial fascia of the orbicularis oculi muscle and its insertion into the galea aponeurosis over the crown of the skull to its connection to the occipitalis, the frontalis muscle exerts its greatest elevation centrally, with its elevation attenuating laterally. The frontalis permits movement of the scalp over the immobile pericranium, elevating the brows and, with overactivity, creates the transverse rhytides of the forehead skin. The nerve supply of the frontalis muscle is the temporal branch of the facial nerve, which travels with the temporoparietal fascia to innervate the frontalis on its undersurface. There is significant variability in frontal branch anatomy, with four branches being a common pattern. Meticulous dissection is the key to avoiding injury, and when operating in the standard planes, clinically apparent nerve injury is exceedingly rare.
Brow Depressors
The procerus is the only midline neuromuscular structure that acts on the brows. With its origin in the fascia of the nasal bones and upper lateral cartilages and its insertion into the skin of the medial lower forehead, the procerus depresses the medial brow, creating the horizontal glabellar rhytides. The procerus is innervated by both the frontal and zygomatic branches of the facial nerve, and therefore selective neurotomy of the frontal branch entering the procerus will have a low rate of long-term success.
The corrugator supercilii is an important determinant of medial brow position. It acts to medialize, corrugate, and depress the medial brow and is responsible for the vertical glabellar furrows. Its origin is the superomedial orbital rim, and its insertion is into the fascia of the lower frontalis muscle and skin of the brow. The supratrochlear and supraorbital neurovascular bundles penetrate through the corrugator muscles on their undersurface before transitioning onto the superficial surface of the frontalis muscle. The main body of the corrugator passes between these two neural structures, anterior to the supraorbital nerve and posterior to the supratrochlear nerve.
The depressor supercilii lies anterior to the supratrochlear nerve. Originating along the medial orbital rim and medial canthal tendon and inserting onto the medial aspect of the bony orbit, the depressor supercilii contributes to medial brow descent. The depressor is located 2 to 3 mm deep and anterior to the corrugator.
♦ Equipment
The necessary equipment for performing endoscopic forehead procedures includes the endoscope, video camera equipment, and surgical instruments. The rigid endoscope is typically between 18 and 23 cm in length, 4 to 5 mm in diameter, and with a 30-degree lens and reversed input light cable. It is equipped with a coupling device to allow visualization on a television screen. Illumination is provided by a halogen or xenon light source according to the surgeon’s preference.
Most endoscopic surgical instrumentation is standardized. However, a few specialized instruments are necessary. The angled endoscopic sheath extends beyond the scope tip, permitting bimanual dissection. The sheath allows saline irrigation of the operative field, which is important to counteract cautery-related cloudiness of the lens without having to remove and wipe the lens during the procedure. While bipolar cautery is usually necessary, monopolar suction cautery is often very helpful. Periosteal elevators may be angled or straight to adjust to various forehead conformations. Sharp-tipped and blunt-tipped elevators should be available to address different degrees of periosteal adherence. A knuckle elevator is useful to dissect over the supraorbital rim. Endoscopic scissors are usually necessary to complete dissection of the dense fibrous tissue over the lateral orbital rim at the brow tail.
♦ Techniques
Brow lifting may be accomplished with a variety of techniques, yet all successful endoscopic procedures share several common features: the use of small vertical incisions, the creation of an optical cavity, the release of the brow complex, and the elevation and fixation of the brow in a more superior position.
Incisions
As endoscopic brow lifting has evolved over the past decade or two, a wide variety of incisions have been used with excellent results. As such, no single pattern may be put forward as representing the ideal. Nevertheless, each pattern of incisions must reflect a considered choice providing adequate access for tissue undermining and soft tissue fixation while keeping the absolute number of incisions to a minimum. Contemporary concepts mandate that the incisions be vertical in orientation, placed in the hair-bearing scalp, starting several millimeters posterior to the non–hair-bearing skin, in the region of nonvillous type hair (Fig. 6.1A, B). The length of the incisions is of lesser importance, as longer incisions may in fact permit less intraoperative tissue trauma and therefore improved healing and postoperative cosmesis than do smaller incisions.
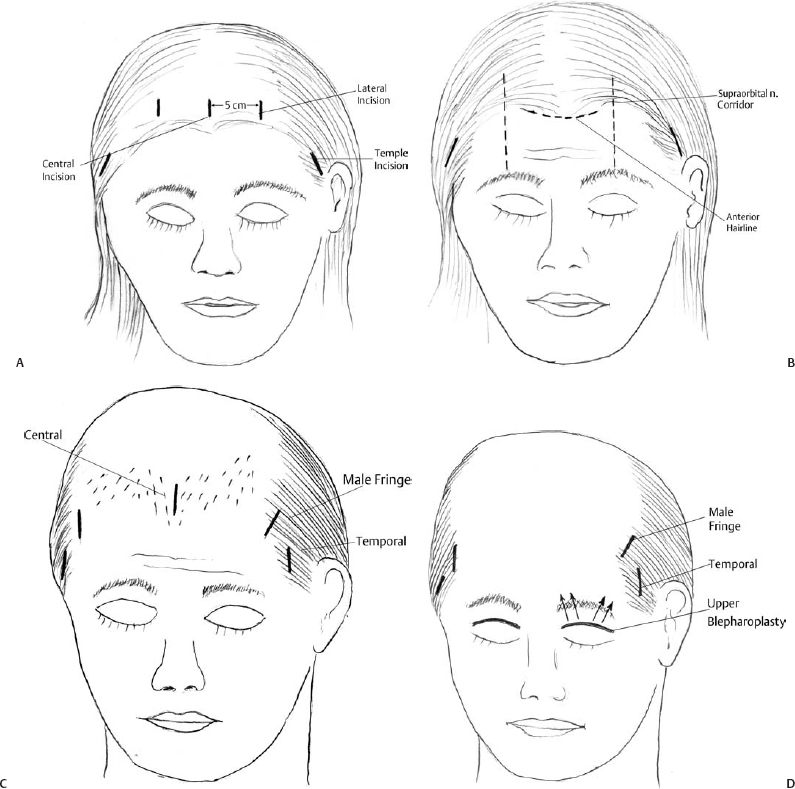
Fig. 6.1 (A) Standard endoscopic forehead incision. (B) Alternate incisions for female patients with high hairlines. (C) Endoscopic forehead incisions for male pattern baldness (Norwood II to V). (D) Endoscopic forehead incisions for male pattern baldness (Norwood VI to VII).
Central Region
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


