Chapter 11 Endoscopic Component Separation 
1 Clinical Anatomy
 The rectus muscle can be fairly wide, up to 8 to 10 cm, and therefore the initial cut down for the balloon dissector must be performed in the lateral abdominal wall to avoid inadvertently placing the balloon in the rectus sheath.
The rectus muscle can be fairly wide, up to 8 to 10 cm, and therefore the initial cut down for the balloon dissector must be performed in the lateral abdominal wall to avoid inadvertently placing the balloon in the rectus sheath.


2 Preoperative Considerations

2 Anatomic Considerations
 Skin Considerations
Skin Considerations
 Skin ulcerations and peristomal excoriations are carefully prepared preoperatively to maximize healing potential. Because skin flaps are not raised in this technique, skin preservation is very important.
Skin ulcerations and peristomal excoriations are carefully prepared preoperatively to maximize healing potential. Because skin flaps are not raised in this technique, skin preservation is very important.
 Musculofascial Considerations
Musculofascial Considerations
 Ideal characteristics for an endoscopic component separation include a relatively wide, well-preserved rectus muscle. With a wide rectus muscle, a large mesh typically can be placed in the retrorectus position as an underlay (as described in Chapter 5 without a skin flap).
Ideal characteristics for an endoscopic component separation include a relatively wide, well-preserved rectus muscle. With a wide rectus muscle, a large mesh typically can be placed in the retrorectus position as an underlay (as described in Chapter 5 without a skin flap).
 Reconstructive Considerations
Reconstructive Considerations
 The surgeon should consider whether skin flaps will be necessary to place the mesh. The absence of skin flaps can create technical challenges in placing a large sheet of mesh as an underlay. If appropriate mesh placement requires large skin flaps, I perform an open technique.
The surgeon should consider whether skin flaps will be necessary to place the mesh. The absence of skin flaps can create technical challenges in placing a large sheet of mesh as an underlay. If appropriate mesh placement requires large skin flaps, I perform an open technique.
3 Operative Steps
1 Equipment
 Equipment needs include a10-mm, 30-degree laparoscope; bilateral inguinal hernia balloon dissector (Covidien, Norwalk, CT); 30-mL balloon-tipped trocar (Covidien, Norwalk, CT); laparoscopic trocars; and an ultrasonic dissector or LigaSure™ device (Covidien, Norwalk, CT) (Fig. 11-1).
Equipment needs include a10-mm, 30-degree laparoscope; bilateral inguinal hernia balloon dissector (Covidien, Norwalk, CT); 30-mL balloon-tipped trocar (Covidien, Norwalk, CT); laparoscopic trocars; and an ultrasonic dissector or LigaSure™ device (Covidien, Norwalk, CT) (Fig. 11-1). Patients receive appropriate preoperative antibiotics and invasive monitoring as needed, and epidural catheters are routinely placed for postoperative pain control.
Patients receive appropriate preoperative antibiotics and invasive monitoring as needed, and epidural catheters are routinely placed for postoperative pain control.


 Trocar Strategy
Trocar Strategy
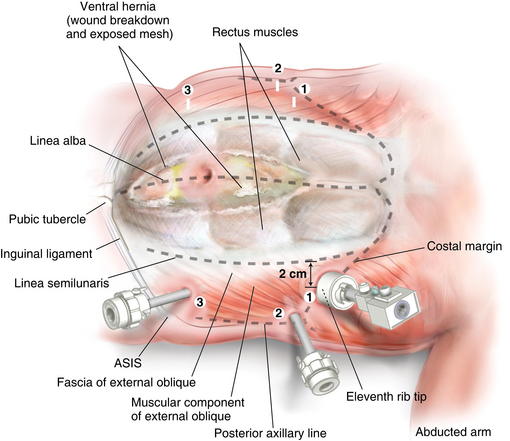
 Figure 11-2 shows trocar positioning, with lines showing the linea semilunaris, external oblique fascia, and costal margin
Figure 11-2 shows trocar positioning, with lines showing the linea semilunaris, external oblique fascia, and costal margin