Chapter 19 Endogenous Growth Factors as Cosmeceuticals
BIOCHEMICAL PATHWAYS OF SKIN AGING
Research in the area of photoaging over the past decade has resulted in an improved understanding of the molecular mechanism of the aging process. Figure 19.1 shows a summary of major pathways involved in the aging process. Absorption of UV radiation by chromophores in the skin as well as cellular oxidative metabolism results in formation of reactive oxygen species (ROS). ROS increase oxidative phosphorylation of cell-surface receptors causing activation of the transcription factor activator protein-1 (AP-1) and nuclear factor kappa B (NF-κB).
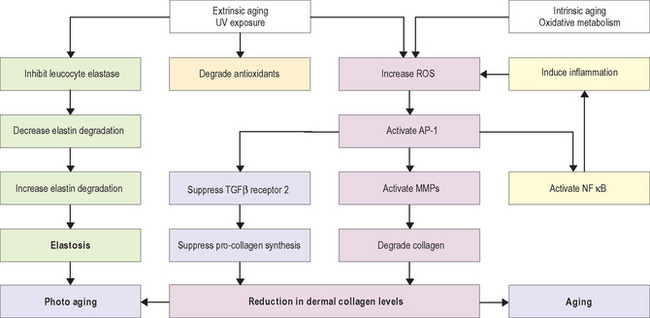
AP-1 stimulates transcription of matrix metalloproteinase (MMP) growth factor genes in fibroblasts and keratinocytes, and inhibits type 1 procollagen gene expression in fibroblasts. MMPs produce degradation of fibrillar type I and type III collagen. Activity of MMP is decreased by binding with tissue inhibitors of metalloproteinase (TIMPs). ROS inactivate TIMPs, thereby increasing MMP activity. AP-1 mediated reduction in synthesis of procollagen appears to result from two mechanisms—interference of AP-1 with type 1 and type 3 procollagen gene transcription and blocking the profibrotic effects of transforming growth factor-beta (TGF-β) by impairment of the TGF-β type 2 receptor/Smad pathway.
GROWTH FACTORS IN WOUND HEALING
Hundreds of growth factors have been identified. Those that are important in wound healing include cytokines involved in immune response and phagocytosis, and growth factors that induce the synthesis of new collagen, elastin, and GAGs (components of the dermal extracellular matrix) that are abnormally affected by UV radiation. Table 19.1 lists the functions of the most important growth factors in wound healing.
Table 19.1 Growth factors in wound healing
| Growth factors and cytokines | Properties/actions |
| Vascular endothelial growth factor (VEGF) | Mediates angiogenesis |
| Chemotactic for endothelial cells | |
| Mitogenic for endothelial cells and keratinocytes | |
| Hepatocyte growth factor (HGF) | Mediates tissue organization and regeneration |
| Platelet-derived growth factor (PDGF) | Chemotactic for fibroblasts and macrophages |
| Mitogenic for fibroblasts, smooth muscle cells, and endothelial cells | |
| Epidermal growth factor (EGF) | Mediates angiogenesis |
| Chemotactic for endothelial cells | |
| Mitogenic for fibroblasts, endothelial cells, and keratinocytes | |
| Granulocyte colony stimulating factor (G-CSF) | Mediates angiogenesis |
| Mitogenic for hematopoietic cells | |
| Transforming growth factor-beta (TGF-β) | Mediates angiogenesis |
| Chemotactic for fibroblasts, keratinocytes, and macrophages | |
| Mitogenic for fibroblasts and smooth muscle cells | |
| Inhibits endothelial cells, keratinocytes, and lymphocytes | |
| Regulates matrix proteins including collagen, proteoglycans, fibronectin, and matrix-degrading proteins | |
| Keratinocyte growth factor | Mediates tissue organization and regeneration |
| Interleukins (IL-6 and IL-8) | Chemotactic for inflammatory cells and keratinocytes |
| Mitogenic for lymphocytes and keratinocytes |
Sources: Fitzpatrick RE, Rostan EF 2003 Reversal of photodamage with topical growth factors: a pilot study. Journal of Cosmetic and Laser Therapy 5:25–34; Moulin V 1995 Growth factors in skin wound healing. European Journal of Cell Biology 68:1–7.
Wound healing is dependent on the synergistic interaction of many growth factors. After injury, cytokines and other growth factors flood the wound site to mediate the inflammatory response, promote new cell growth, and decrease wound contraction and scarring. The process of wound healing is commonly divided into four overlapping phases that describe physiologic responses to injury. These phases include hemostasis, inflammation, proliferation, and remodeling. Figure 19.2 summarizes each phase of wound healing along with dominant growth factors and cytokines. During hemostasis, platelets release various cytokines and other growth factors at the wound site to promote chemotaxis and mitogenesis. In the inflammatory stage, neutrophils and monocytes migrate to the wound site in response to specific cytokines and growth factors to initiate phagocytosis and to release additional growth factors that will attract fibroblasts. The proliferation phase is marked by epithelialization, angiogenesis, granular tissue formation, and collagen deposition. During proliferation, keratinocytes restore barrier function to the skin and secrete additional growth factors that stimulate the expression of new keratin proteins. Fibroblasts produce collagen that is deposited in the wound bed. This cycle of collagen production and growth factor secretion continues in a type of autocrine feedback loop of continuous wound repair.
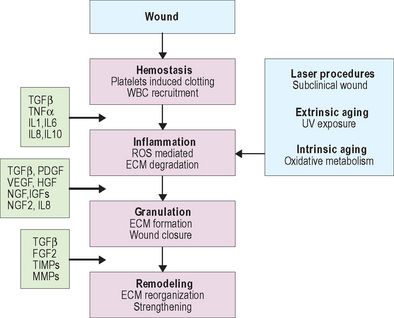
The remodeling phase is the final step in the wound repair process and typically lasts several months. It is during remodeling that the extracellular matrix is reorganized, scar tissue is formed, and the wound is strengthened. Type III collagen deposited during the proliferation phase is gradually replaced by type I collagen, which is more tightly cross-linked and provides more tensile strength to the matrix than type III collagen. Cells at the wound site secrete several growth factors with specific functions related to remodeling and matrix formation. For example, collagen and fibronectin synthesis are initiated by TGF-β, while PDGF and TGF-β stimulate fibroblasts to produce GAGs and modulate the proliferation of smooth muscle cells. Other growth factors modify the vasculature. Over time, cell density increases and skin tissue is strengthened.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


