(1)
Wound Healing Unit, Department of Surgery, Montpellier University, Montpellier, France
6.1 Introduction
Electrical burns are rare but can be particularly severe or injuring and sometimes fatal. They represent approximately 5 % of burns [1]. In addition, it is estimated that 4,000 people every year undergo an electrocution in France.
This type of burn affects mainly two categories of patients:
The young child exploring his environment
The adult in his workplace
They are two types:
Damage by direct contact with the electric current. The lesions spreading from an entry point to an exit point of the current (our focus of interest in this chapter).
Injury by electric arcs in accidents at very high voltage. That is mainly thermal burns but at a very high temperature (>2,000 °C).
They can be divided into two groups:
Low voltage injuries (<1,000 V) occurring mainly at home
High voltage injuries (>1,000 V) occurring more often in the workplace
They mainly concern two locations:
The upper limb
The face
Mechanisms of tissular injury appear to be of three different types:
The Joule effect: generating heat depending on tissue resistance – “J = R I2 T”. The amount of the heat intensity generated (J depends indeed on voltage U because U = RI. T is the duration in seconds of the contact, R is the resistance in ohms, and I is the intensity in amperes).
The higher the resistance, the greater the heat generated will be and the more serious the injuries are, but less current will travel through.
Actually two parameters influence tissue resistance:
Its category (with decreasing resistance): Bone > fat > skin > muscle > mucosa > vessel > nerve
Its diameter: the smaller the diameter (wrist, elbow and ankle), the higher the resistance, and thus the damage related to the Joule effect is significant [2].
Cell membrane destruction by electric shock (electroporation) [3] increasing tissue damage and promoting the release of myoglobin.
Massive depolarisation, which will result in the damage of muscle, cardiac and nervous cells. The “shock” causes phenomena of tetanisation, which increase the contact time of the victim with the electric current source (cable grasps, feeling of being “stuck” to the source). Furthermore, tetanisation allows the joint’s jump of current by hyperflexion of the joints [4].
6.2 Tissue Injury
1.
Entry and exit skin points
These points are most often located at the extremities. The entry point is centred by a sore indicating carbonisation. This area is surrounded by a burn of decreasing depth (“cockade aspect”). On the way to the exit point, an area of deep burn should be suspected, following theoretically the path of sensory and motor nerves (the superficial veins also).
However, the current path remains unpredictable. Meanwhile, the exit point more often represents a whitish area. During the impact, it links the body to the ground or other external elements connected to it (Fig. 6.1).
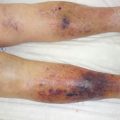
Fig. 6.1
Example of multiple points of entry and exits in the same patient
2.




Muscle injury
It is always more severe than suggested by skin lesions and is due to the action of depolarisation and Joule effect. It represents the most important vital and functional prognosis factor in this type of burn. Muscles submitted to high voltage will undergo a very significant oedema, which can lead quickly to a compartment syndrome (>30 mmHg). This syndrome, if not managed by a fasciotomy, will significantly increase muscle, nerve and vascular damage, by direct compression, thrombosis [5] and necrosis leading to local acidosis. This vicious cycle is to be broken as soon as possible (Fig. 6.2).

Fig. 6.2
Carbonisation of upper limb responsible for major and composite tissue lesions
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
