Chapter 3 Dynamics of Rhinoplasty
Online Contents
 Animations
AnimationsIn this Chapter Online at experconsult.com
Deepening the Radix Elongates the Nose Animation 3.1
Augmenting the Radix Elongates the Nose Animation 3.2
Transposing the Nasal Bones and ULCs by Osteotomy Animation 3.3
Removing the Cephalic Margin of the LLCs Increases the Distance Between the Domes Animation 3.4
Lowering and Reconstructing the Domes Restores the Normal Configuration of the Tip Animation 3.5
Overlapping the Lateral and Medial Crura Sets the Domes Back Without Rotation Animation 3.6
Reducing the Nasal Spine and Anterocaudal Septum Results in the Loss of Tip Projection Animation 3.7
Interdomal Sutures Approximate Domes That are too Far Apart Animation 3.9
Improving a Narrow, Assymetrical Tip with a Subdomal Graft Animation 3.10A, B
Augmenting Tip Projection with Tip Graft and a Columella Strut Animation 3.11A, B
Increasing Tip Projection by Inserting an Anchor Suture Animation 3.12
A Wedge of Caudal Septum is Removed to Rotate the Tip Cephalically Animation 3.15
Cephalic Rotation of the Tip Using a Wedge Resection Animation 3.16
Removing the Cephalic Margin of the LLSs Rotates the Tip Cephalically Animation 3.17
Pearls
• Different means of achieving the same objectives have their own minor nuances and may entail unexpected additional changes. This makes a precise understanding of rhinoplasty dynamics essential for a successful outcome.
• Cephalic deepening of the radix will result in elongation of the nose while deepening at the level of the canthus, and caudal to it, may make the nose appear shorter.
• Deepening of the radix will induce the appearance of an increased intercanthal distance.
• Augmentation of the radix will render an appearance of reduced intercanthal distance.
• Reduction of the dorsum will engender an appearance of a wider nose while its augmentation will result in a nose that appears narrower.
• Osteotomy of the nasal bones will result in the appearance of a narrow nose and a decrease in intercanthal distance.
• Osteotomy and medial repositioning in the nasal bone may result in medialization of the upper lateral cartilage. The longer the nasal bone, the greater the effect that will be transferred to the upper lateral cartilage.
• When the cephalic margin of the lower lateral cartilages is trimmed, the domes will be separated, resulting in bossae. Furthermore, the tip will slightly rotate cephalically and if the resection is aggressive, it can result in retraction of the ala. Placement of an interdomal, lateral crura spanning, or medial genu suture will prevent this.
• Removal of the cephalic margin of the lower lateral cartilages, lowering or removal of the domes, transection of the lateral crura, medial crura, or both, tip setback anchor suture, lowering the anterocaudal septum, nasal spine reduction, and maxillary setback will all result in reduction in tip projection.
• A tip narrowing can be achieved through interdomal, transdomal, lateral crura spanning, and anterior medial crura sutures. The tip can also be narrowed using a tip graft and domal interruption as a last resort.
• The tip can be widened through an interdomal or subdomal graft A wide onlay graft can be used if the aesthetics of the nose make it advisable.
• Increase in tip projection can be achieved through a tip graft, columella strut, transdomal suture, approximation of the footplates, medial crura anchor suture to the anterocaudal septum, nasal spine augmentation, maxillary advancement, and Fred technique.
• Cephalic rotation of the tip can be achieved through anterocaudal septum resection along with the membranous septum reinforced with a tip rotation suture, removal of the cephalic margin of the lower lateral cartilages, placement of columella strut, footplate approximation, and nasal spine augmentation.
• Nasal dorsal reduction may provide an optical illusion that the tip has been rotated cephalically.
• A nasal spine graft will result in shorter upper lip, an increase in tip projection and widening of the nasolabial angle.
• Reduction of the nasal spine will result in a longer appearance of the upper lip, narrowing of the nasolabial angle, and reduction in tip projection.
• Approximation of the footplates will result in augmentation of the tip projection, narrowing of the base of the columella, and slight cephalic rotation of the tip, and caudal advancement of the subnasale.
• Reduction of tip projection can result in widening of the alar base and bowing of the columella caudally.
• Narrowing of the alar base will not only result in reduction of the nostril width, it will also transpose the alar rim caudally.
• Placement of the alar rim graft will eliminate alar concavity, reposition the alar rim caudally, increase the nostril length and widen the nostril which will improve the function of the external valve.
One of the factors that makes rhinoplasty a continuous challenge is the complicated dynamic interplay that occurs with each maneuver, resulting in additional changes that may or may not be in agreement with the aesthetic goals.1–2 When a number of maneuvers are carried out simultaneously, the associated changes with each maneuver become difficult to predict, thus creating an enigma for the surgeon. Knowledge of these effects garnered through experience and reading the related literature will ultimately lead to more predictable rhinoplasty outcomes.
The Radix
Depending on how cephalad the deepening of the radix is, a different outcome can be expected (Figure 3.1; Animation 3.1). More cephalad deepening will result in elongation of the nose, while deepening at the medial canthus or caudal to it will produce a shorter appearance in the nose. This is very intriguing in that both augmentation and reduction can potentially make the nose look long, depending on the site of deepening (Figure 3.2; Animation 3.2). Deepening of the radix will induce the appearance of an increased intercanthal distance.
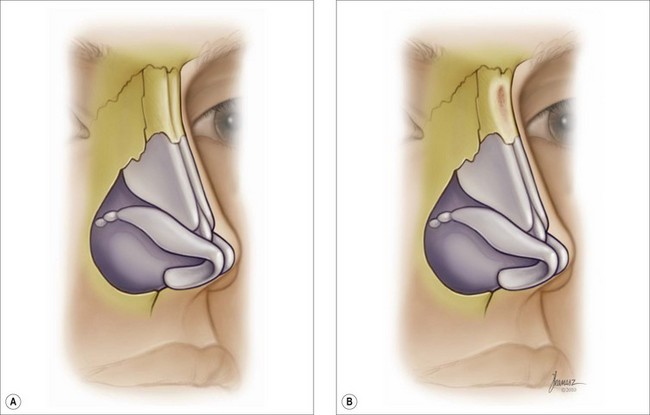
Figure 3.1 As the radix is deepened, if the deepening is cephalad, it will result in elongation of the nose. 

 Animation 3.1 •
Animation 3.1 • Animation 3.2 •
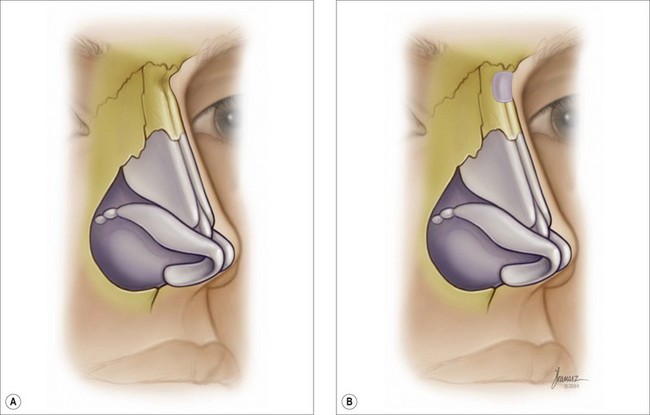
Animation 3.2 •The Dorsum
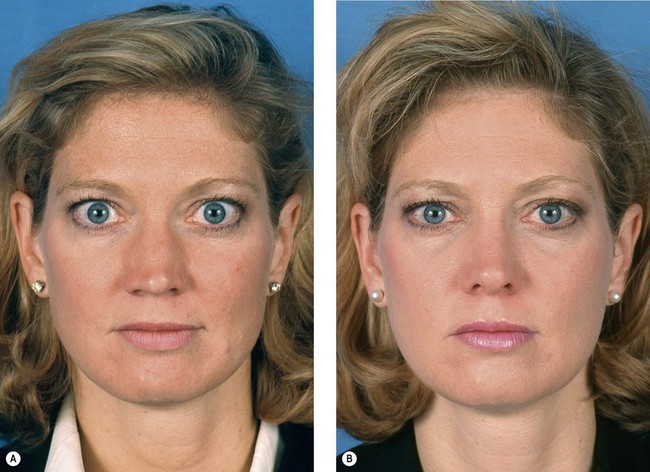
The presence of a dorsal hump provides the appearance of a narrower bridge. As the hump is removed, the dorsum will appear wider even after an osteotomy and narrowing of the distance between the nasal bones (Figures 3.2, 3.3). Additionally, removal of the dorsal hump provides an appearance of increased intercanthal distance. Augmentation of the dorsum will have a reverse effect: the dorsum will look narrower and the intercanthal distance will appear shorter as long as the graft utilized is not too wide (Figure 3.4). Osteotomy of the nasal bones will result in the appearance of a narrower nose and a decrease in the intercanthal distance (Figure 3.5).


Furthermore, osteotomy and medial transposition of the nasal bone and the upper lateral cartilage (ULC) may also reduce the nasal airway. However, this change will be more drastic when the nasal bones are longer, which will have more influence on the ULC (Figure 3.6; Animation 3.3) if the nasal bones are transposed medially to a significant degree (Figure 3.7) or if the inferior turbinate extends anterior to the plane of osteotomy (Figure 3.8). To avoid medialization of the inferior turbinates, one may start the osteotomy more anteriorly or do a high to low osteotomy (Figure 3.9). Alternatively, one may perform a conservative inferior turbinectomy.3 Avoiding an osteotomy is an option, but in most instances this is not an acceptable aesthetic compromise. Furthermore, in order to reduce the ill effects of the medialization of the ULC on the nasal valve and dorsal aesthetic lines, insertion of spreader grafts may become necessary. If the removed dorsal hump is small enough to avoid an open nasal roof, spreader grafts may not be necessary unless there is a primary internal valve dysfunction. When removal of a small dorsal hump results in minimal opening of the roof, preservation of the mucoperichondrium may make it unnecessary to use spreader grafts to prevent medialization of the ULC. However, whenever a large dorsal hump is removed, it invariably results in medial transposition of the ULC, which may not be initially discernible. It may take between 6 months and a year for the inverted ‘V’ deformity to become visible. It is thus prudent to use bilateral spreader grafts or flaps whenever a large dorsal hump is removed. While in most instances spreader grafts will be sufficient, in rare cases when the ULCs are extremely short or attenuated a splay graft may provide a better functional outcome.4



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


