Chapter 4 Disorders of keratinization
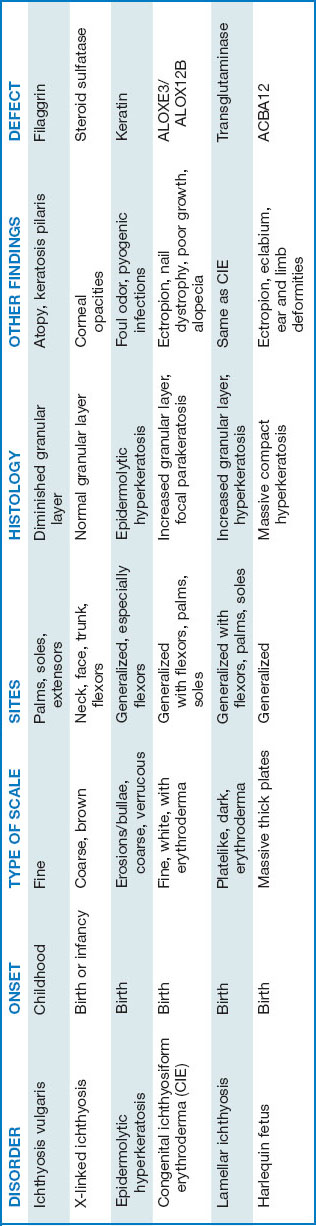
Ichthyosis vulgaris (Fig. 4-1A,B) usually develops around school age, and is characterized by generalized xerosis and scale, with characteristic sparing of the flexural skin. Additional findings include follicular accentuation (keratosis pilaris), hyperlinearity of palms and soles, and a personal or family history of atopy. Rare patients may have an associated palmar-plantar keratoderma. Skin biopsy demonstrates a decreased granular cell layer associated with moderate hyperkeratosis.

X-linked ichthyosis, in contrast, is usually present by one year of age, affects the posterior neck with “dirty”-appearing scales, and spares the palms and soles (Fig. 4-1C). The skin changes—gradually worsening with age—with the neck, face, and trunk ultimately developing thick, brown scales. The disease is caused by a defect in steroid sulfatase, an enzyme important in cholesterol synthesis and vital for normal development and function of the stratum corneum. Accumulation of cholesterol sulfate and a lack of tissue cholesterol ensue, leading to a disturbance in steroid hormone metabolism. Skin biopsy of X-linked ichthyosis is rarely diagnostic, and demonstrates a normal granular layer with hyperkeratosis.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


