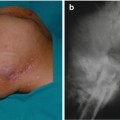
Fig. 14.1
AP pelvis of a patient showing bilateral previous Girdlestone procedure and destruction of both ischial bones with a thin pelvic bone prior to previous disarticulation
Fig. 14.2
X-ray of AP pelvis of the same patient with previous disarticulation of the right hip, and the patient is for left disarticulation procedure. Notice the destruction of the pelvic bone architect
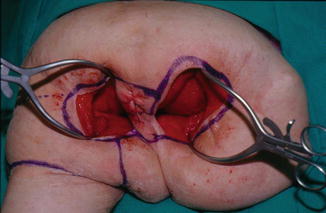
Fig. 14.3
Operative photograph showing extensive bilateral ischioperineal ulceration involving the anus with previous disarticulation and total thigh flap on the right side with previous multiple flaps
Fig. 14.4
Operative photograph showing patient in prone position with the marking for amputation and disarticulation
Fig. 14.5
Operative photograph of patient in prone position lateral view showing the lateral marking for the dissection of the entire femur; the marking is over the scar of the old Girdlestone procedure
Fig. 14.6
Operative photograph showing that the entire femur was dissected from the entire thigh and amputation was performed above knee level and dissection to excise the anus

Fig. 14.7
Operative photograph showing the entire femoral shaft which was dissected and attached to the knee and leg. The entire specimen was sent for pathology
Fig. 14.8
Operative photograph of close-up view showing the dissection to excise the anus and closures of the rectum in this case. Arrow indicates location of rectal stump
Fig. 14.9
Operative photograph showing excision of the skin of the posterior thigh flap to expose a group of muscle to be insetted into the defect
Fig. 14.10
Operative photograph showing the insetted muscle part of the total thigh flap in the defect

Fig. 14.11
Operative photograph showing complete closure of the total thigh flap to cover the entire defect

Fig. 14.12
Postoperative photograph 6 weeks post surgery showing complete healing of the flap
Case 2
Fig. 14.13
Photograph of a spinal injury patient presented with extensive necrosis and infection of the entire gluteal and trochanteric area

Fig. 14.14
Operative photograph of the same patient in prone position about 4 weeks post debridement and wound care (right lateral view)

Fig. 14.15
Operative photograph of the same patient in prone position showing the extent of the ulcer with evidence of previous multiple flaps. Few weeks post debridement of the extensive ulceration

Fig. 14.16
Operative photograph of the same patient in prone position showing the extent of ulceration (left lateral view)

Fig. 14.17
X-ray of AP pelvis of the same patient showing heterotopic ossification of the right hip with ankylosis, which is one of the indications to perform disarticulation of the right limb

Fig. 14.18
Operative photograph postsurgical debridement of the entire ulceration
Fig. 14.19
Operative photograph lateral view showing the exposure of the entire femoral shaft and the hip heterotopic ossification (H.O.) through a lateral approach
Fig. 14.20
Operative photograph lateral view showing the amputation at above-knee level and the dissection of the entire total thigh flap from the femoral shaft
Fig. 14.21
Operative photograph of patient in prone position post complete disarticulation of the entire femur and hip H.O. excision from the total thigh flap
Fig. 14.22
Operative photograph of patient in prone position, post insetting of the total thigh flap to cover the entire open areas

Fig. 14.23
Photograph of 6 weeks post total thigh flap showing complete healing (patient in prone position)
14.3 Modification of Total Thigh Flap Procedure
14.3.1 Excision of the Anus and Rectal Closure
As mentioned previously, to inset the total thigh flap across the sacrococcygeal area, anatomically, the anus will be in the pathway of the total thigh flap inset. In this circumstance, there is indication to excise the anus and close the rectum, preoperatively. If the type of colostomy is not known, a special radiological test should be done by injecting a Gastrografin radio-opaque dye either through the colostomy or the anus and taking X-rays which will demonstrate the type of colostomy the patient has. If the colostomy is not a double loop, the general surgeon will need to perform a mucous fistula by bringing the defunctioning loop of the sigmoid colon to the abdominal wall prior to the total thigh flap surgery. The excision of the anus is done by marking the incision around the anus with the electrocautery around the anal verge; then the incision is deepened and tissue clamps are placed over the mucocutaneous junction. The dissection continues around the anus to dissect it from the soft tissue for a length of 6–8 cm; then the anus is transected from the rectum. Tissue clamp is placed around the rectal edges, and then the rectal stump is closed by two layers; the first layer is by through-and-through continuous stitches by using 3-0 Vicryl suture on GI needles, and then the invagination of this layer is by the seromuscular layer closure. Using the same type of sutures, the rectum is dropped in the cavity and soft tissue is closed over the stump. If the gracilis muscle was not used previously, it can be utilized to cover the rectal stump. Then the total thigh flap is insetted to cover the defect area including the excised anal area (Figs. 14.24, 14.25, 14.26, 14.27, 14.28, and 14.29), showing the operative procedure of the anal excision during disarticulation and total thigh procedure.

Fig. 14.24
Operative photograph showing patient in prone position with multiple extensive stage IV ulcer involving the anus. Patient with history of multiple flap surgery in the past with the only option available to disarticulate and total thigh flap and closure of the anus. Arrow indicates anus position
Fig. 14.25
Operative photograph of the same patient in a lateral view
Fig. 14.26
Operative photograph showing post-excision of all the ulcers showing the incision around the anus with traction on the anal verge to start dissection around the anus
Fig. 14.27
Operative photograph showing complete dissection around the anus; the transection of the anus and closure of the rectal stump in layers was performed
Fig. 14.28
Operative photograph showing post closure of the rectum and post disarticulation and total thigh flap
Fig. 14.29
Operative photograph showing the complete insetting of the total thigh flap covering the entire defect and the rectal closure area and completely sutured in layers
14.3.2 The Extended Total Thigh Flap (Below the Knee)
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


