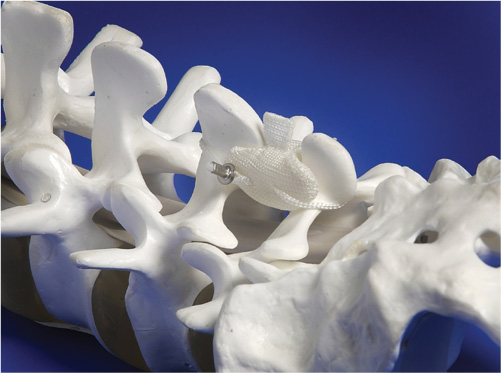
35 Spinal arthrodesis is frequently used to treat syndromes related to degenerative pathologies of the lumbar spine.1–6 Inconsistent clinical results as well as substantial morbidities and complications have been reported following lumbar arthrodesis.7–10 Biomechanical studies have suggested that the restriction of segmental motion resulting from spinal fusion causes abnormal kinematics at adjacent mobile segments, potentially leading to instability and accelerated degeneration at these levels.11–13 In an attempt to eliminate problems innate to fusion surgery, the concept of dynamically stabilizing a diseased lumbar motion segment has been proposed. Theoretically, dynamic stabilization preserves lumbar motion while reducing abnormal painful movement.13,14 Total disk arthroplasty has been advocated as a motion-restoring treatment for pain arising from the intervertebral disk. Alternatively, posteriorly implanted, motion-limiting devices that reduce but do not eliminate motion have been widely investigated in Europe for the treatment of mechanical back pain and spinal stenosis.15–18 Posteriorly-based, dynamic devices include (1) pedicle systems with tethers between the intrapedicular anchors and (2) interspinous process devices. The first-generation interspinous process implant for non-rigid, lumbar stabilization was developed in 1986.18 Over the past 20 years, several designs of interspinous process devices have been developed; however, the clinical indications for their use remain poorly defined. The clinical results with these devices have been reported only in anecdotal case reports, with varied indications and incomplete patient follow-up making meaningful interpretation difficult. The Device for Intervertebral Assisted Motion (DIAM; Medtronic Sofamor Danek, Memphis, TN) is a silicone interspinous process “bumper” designed to provide facet distraction, decrease intradiskal pressure, and reduce abnormal segmental motion and alignment. The rationale for an interspinous spacer dynamic stabilizing device should be based on lumbar biomechanics and anatomy. In the healthy spine, the majority of the compressive load is transferred through the anterior column, whereas only 18% is supported posteriorly by the facet joints.19,20 Anterior compressive forces are distributed uniformly in simple and eccentric loading.21–25 As the disk degenerates, however, nonuniform stress distributions can develop in eccentric loading, and the disk exhibits properties more characteristic of a solid.19,26 Stress concentrations are directed toward the outer annulus and away from the nucleus. Advancing degeneration shifts load to the posterior elements of the spine.27–29 Yang and King indirectly measured facet forces and demonstrated a significant increase in facet load for segments with degenerated disks.30 The increase in facet load was greater as the eccentricity of the posteriorly applied compressive load increased. The facet joints have an absorbing and stabilizing role,31 with the axis of motion centered along the junction of the spinous process and lamina.11,12 As disk degeneration progresses and anterior column support is lost, the facet joints bear more weight and the motion segment fulcrum moves dorsally.32 Additionally, as the disk degenerates, it loses its biomechanical competence so that the facet joint becomes the primary restraint to translational and torsional moments across the involved motion segment.33–35 This increased load concentration within the facet joints may accelerate facet degeneration and increase the likelihood of facet-mediated pain.36,37 Theoretically, an interspinous device should assist in the functioning of the diseased motion segment by providing stability and load-sharing the axial forces transmitted through the posterior elements. As such, if an elastic device is to be implanted to restore facet function its placement should be posterior.16,17,32,38,39 The preloading of the implant should permit posterior tensioning restoring natural ligamentotaxis. An ideal shock absorber would be radiolucent and would display a nonlinear behavior in compression.7,32,40 The DIAM Spinal Stabilization System is a silicone “bumper” that is inserted between the spinous processes (Fig. 35–1). It acts as a shock absorber and displays nonlinear behavior.17,40 The DIAM is designed to dynamically support the vertebrae while also maintaining distraction of the foramina. The DIAM will also restore posterior column height and share in load transmission, thereby theoretically relieving stresses on both the anterior and posterior elements of the spine. As a result of its interspinous position, the DIAM serves to realign the facet interface restoring its congruence (Fig. 35–2A,B). It is important to realize that the DIAM is designed to dampen the existing painful motion of the involved segment, whereas disk arthroplasty restores motion of a degenerated spinal segment. The DIAM behaves as a pivot point for achieving spinal “balance.”7 With the DIAM implanted, resistance to flexion is controlled first by the stretching of the DIAM cable, followed by stretching of the posterior musculoligamentous structures. During extension, the DIAM continues to be loaded until reaching its limit of compressibility.17,38,39 The deformability of the DIAM device allows for stress to be distributed evenly over the bony anatomy as opposed to a more rigid device. The deformability also serves to preserve motion in a passive capacity, reducing the potential for altered kinematics. Figure 35–1 DIAM (Device for Intervertebral Assisted Motion) Spinal Stabilization System is a silicone “bumper” that is inserted between the spinous processes. (Image courtesy of Medtronic Sofamor Danek, Memphis, TN, 2004.) Indications for the DIAM remain poorly defined and largely reflect individual surgeon biases. It would appear that the DIAM has been used in cases of disk herniation, spinal stenosis, and facet syndrome and disk dysfunction, and to dampen kinematic changes at levels adjacent to a fusion (known as topping off). Hemilaminotomy and diskectomy are frequently used for the treatment of a symptomatic herniated disk. Although diskectomy is quite effective in relieving radicular symptoms, persistent mechanical low back pain is not uncommon.33 Postdiskectomy back pain likely relates to underlying disk degeneration as well as the altered kinematics at the involved segment. Biomechanical studies have confirmed that a hemilaminotomy, partial diskectomy does indeed cause increased segmental angular motion over that seen in the intact state.12,14 This nonphysiological motion may lead to altered stresses across the motion segment stabilizers, including the intervertebral disk, facet joints, and supporting musculoligamentous structures.41 In a human cadaveric study, Phillips et al showed that the DIAM tends to normalize the altered motion segment kinematics seen after diskectomy.14 Acquired stenosis is the most frequent cause of neurogenic claudication. Retrolisthesis may worsen the stenosis. Implantation of the DIAM may effect indirect neural decompression by placing the motion segment in slight flexion, thereby increasing the spinal canal and neuroforaminal dimensions. In addition, the DIAM may mitigate dynamic stenosis by reducing motion of the involved segment. Although DIAM implantation may indirectly relieve foraminal stenosis or stenosis arising from soft tissue compression, it has been more typically combined with limited direct neural decompression. Dysfunction of the disk leads to posterior transfer of the loads to the facet joints.19 The DIAM may play a role in preventing pain resulting from overloading of the facet joints by off-loading the facets and reducing motion.15,16,38 Findings of facet dysfunction or overloading include the presence of hypertrophic facets, synovial cysts, and facet incongruity, which may also be inferred from laxity of the posterior inter-spinous ligaments with abnormal approximation of the spinous processes.42,43 Taylor et al have described signs of posterior load transfer, including retrolisthesis and hyperlordosis, across the disk and have suggested these as possible indications for placement of DIAM at the time of diskectomy14,32,40,44 (Fig. 35–3A–C). Another potential application of the DIAM might be to dampen the changes in kinematics imposed at the levels adjacent to a fusion. Several authors have reported increased motion at the unfused segments above a fusion with the application of compressive and bending loads.45 Similarly Shono et al reported significant increases in flexion-extension, axial rotation, and lateral bending at the segment adjacent to a single- or two-level pedicle screw construct.46
DIAM (Device for Intervertebral Assisted
Motion) Spinal Stabilization System
Biomechanics
DIAM
Mechanism
Indications
Disk Herniation
Spinal Stenosis
Facet Syndrome and Disk Dysfunction
Topping Off
Related posts:
 Prosthetic Disk Nucleus Partial Disk Replacement: Pathobiological and Biomechanical Rationale for Design and Function
Prosthetic Disk Nucleus Partial Disk Replacement: Pathobiological and Biomechanical Rationale for Design and Function
 Complications of Lumbar Disk Arthroplasty
Complications of Lumbar Disk Arthroplasty
 Tension Band System
Tension Band System
 Cervidisc Concept, Six Years Follow-Up and Introducing Cervidisc II: DISCOVERY
Cervidisc Concept, Six Years Follow-Up and Introducing Cervidisc II: DISCOVERY
 Rationale for Dynamic Stabilization
Rationale for Dynamic Stabilization
![]() Nonfusion Stabilization of the Degenerated Lumbar Spine with Cosmic
Nonfusion Stabilization of the Degenerated Lumbar Spine with Cosmic
![]()
Stay updated, free articles. Join our Telegram channel
 Biomechanics
Biomechanics DIAM
DIAM Contraindications
Contraindications Surgical Considerations
Surgical Considerations Discussion
Discussion Conclusion
Conclusion
Full access? Get Clinical Tree


