© Springer-Verlag Berlin Heidelberg 2015
Renato G. Panizzon and M. Heinrich Seegenschmiedt (eds.)Radiation Treatment and Radiation Reactions in Dermatology10.1007/978-3-662-44826-7_1515. Diagnosis and Treatment of Cutaneous Radiation Injuries
(1)
Capio Blausteinklinik, Hospital for Vascular Surgery and Dermatology, Erhard-Groezinger-Strasse 102, Blaustein, D-89134, Germany
15.1 Epidemiology
15.3 Clinical Findings
15.4 Diagnostic Approach
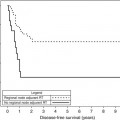
15.5 Course and Prognosis
15.6 Therapy
15.1 Epidemiology
Individuals are exposed to ionizing radiation either intentionally during radiation therapy, most often for systemic or cutaneous malignancies, through industrial exposure, or following a major accident such as at Chernobyl, Lilos [4–8], or, recently, Fukushima. In the past, hospital workers were at risk, as the dangers of ionizing radiation were not fully appreciated; recently, new diagnostic procedures in cardiology pose a new risk pattern [9].
However, while accidents are still the most common source, the concern is about the intentional misuse of nuclear materials in the realm of international terrorism or organized crime. Possible scenarios include:
Detonation of a small nuclear explosive in a densely populated area
Adding radioactive nuclides, usually with a short range, to a conventional explosive
Hiding radioactive substances in objects of daily use such as chairs or car seats for the elimination of a single individual
15.2 Aetiology and Pathogenesis
In all these scenarios, there will be an inhomogeneous exposure to particles of varying injuries with a surface skin dose of 60–100 Gy or more. Depending on the nature of the nuclides, there may be a sharp drop in dosage after several cm so that lethal dosages are unlikely to reach the bone marrow. Thus, the skin is likely to be the organ most severely affected. This is true not only for α- and β-rays but also for sources dominated by γ-rays, such as 137Cs and 60Co. Characteristic for such exposure is that initially inadequate attention is paid to ionizing radiation so that early or abortive signs and symptoms are often overlooked. The physician is paradoxically faced with patients who present with acute damage days or weeks after exposure. A thorough understanding of the course of the pathophysiologic reaction is essential for prompt diagnosis and appropriate therapy.
Ionizing radiation is best known for inhibiting proliferation of stem cells in tissues which are otherwise capable of regeneration, such as the skin, mucosa, and bone marrow. In addition, it elicits transcription of a cascade of proinflammatory cytokines (IL-1, IL-3, IL-5, IL-6, TNF-α), chemokines (IL-8, eotaxin, CCR-3 receptor), receptor tyrosine kinases (EGF-R), and adhesion molecules (ICAM-1, VCAM, E-selectin) in keratinocytes, fibroblasts, and endothelial cells. These factors combine to create a local inflammatory reaction rich in neutrophils and eosinophils, which is self-perpetuating, leading to marked tissue damage [2, 3].
The pathophysiology of early and late damage from ionizing radiation is quite different. The early reaction in the first few days reflects the immune activation and inflammation, while the late reaction after weeks underscores the damage to the epidermal stem cells and resultant loss of protective covering. Later, the main change is the expression of TGF-beta1 in dermal and subcutaneous fibroblasts with overproduction of collagen. Thus, the late radiation changes represent a lymphocytic fibrotic inflammation.
15.3 Clinical Findings
The term cutaneous radiation syndrome (CRS) was proposed by the Second Consensus Development Conference for the Diagnosis and Treatment of Radiation Injuries in 1993 to compass the complex series of events that follow exposure to ionizing radiation and has in the meantime received general international acceptance (recent query in Google: more than 68,000 hits) The following clinical stages can be identified:
Prodromal erythema. In this brief phase, lasting minutes to hours, there is erythema and pruritus, which resolves and is followed by a latent period.
Acute or manifest. This is equivalent to the old term of acute radiation dermatitisRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree