Dental‐Occlusal Relationships: Terminology, Description and Classification
Chapter 22 Dental‐Occlusal Relationships: Terminology, Description and Classification
Introduction
A thorough understanding of ‘ideal’ and normal functional dental‐occlusal relationships, together with the relationship of the dentoalveolar complex to the craniofacial complex, is paramount for accurate facial aesthetic evaluation and subsequent clinical diagnosis.
Terminology
The description of the structural relationships of the teeth and the dental occlusion, as with the rest of the craniofacial complex, is impossible without an understanding of the specialized vocabulary.
Terms of description of tooth form
There are 20 teeth (10 per jaw) in the deciduous or primary dentition. There are 32 teeth (16 per jaw) in the complete permanent dentition. In both dentitions there are three basic tooth forms:
Incisiform: These are cutting teeth, which have thin, blade‐like crowns.
Caniniform: These are piercing or tearing teeth, which have a single, robust, pointed, cone‐shaped crown; canine teeth are sometimes termed ‘cuspid’ teeth.
Molariform: These are grinding teeth, which possess a number of cusps on an otherwise flattened biting surface. Premolar teeth are sometimes termed ‘bicuspid’ teeth.
Other terms of description are:
Anatomical crown: The portion of a natural tooth that extends coronal from the cementoenamel junction (CEJ).
Clinical crown: The portion of the tooth crown visible in the oral cavity, extending from the cusp tip or incisal edge to the free gingival margin.
Root: The portion of a tooth apical to the CEJ that is normally covered by cementum (anatomical root) and is attached via the periodontal ligament to the supporting alveolar bone (clinical root).
Cervical margin: The junction of the anatomical crown and root.
Occlusal surface: The biting surface of the molar and premolar teeth.
Incisal edge: The cutting edge of the incisor edge.
Cusp: A cone‐shaped prominence on the crown of a tooth, forming the occlusal surface.
Cingulum: A lingual/palatal lobe of some anterior teeth (incisors and canines) in the form of a convex protuberance on the cervical one‐third of the lingual/palatal surface of the anatomical crown.
Marginal ridge: A linear elevation on the mesial or distal edge of the occlusal surface of molariform teeth.
Fossa: An anatomical depression in the occlusal surface of a tooth.
Fissure: An anatomical cleft or groove between cusps or ridges on the occlusal surface of a tooth.
Terms of direction in dental nomenclature
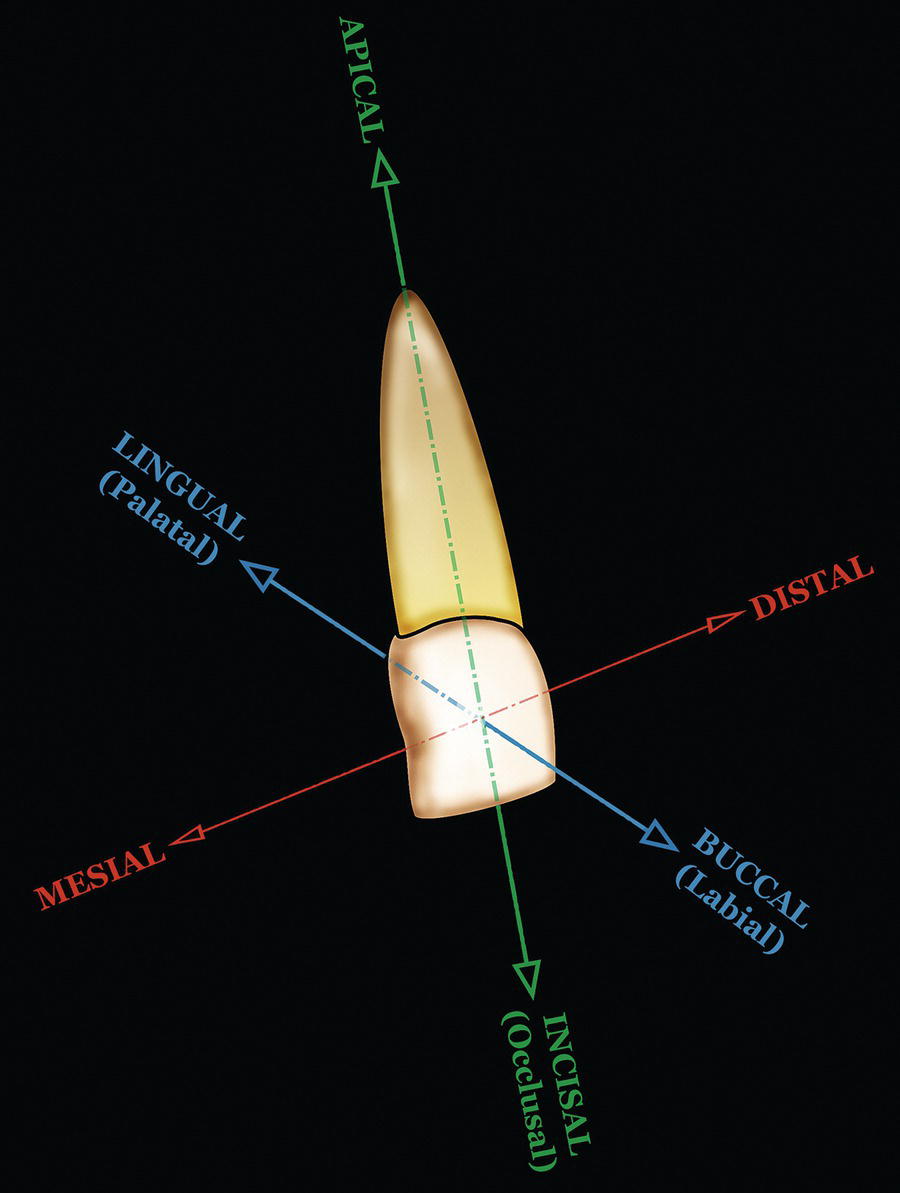
Basic dental directions may be described in terms of orientation in relation to the teeth. The following terms may be used to describe both the tooth crown surfaces and directions of tooth movement (Figure 22.1):
Figure 22.1 Terms of direction in dental nomenclature may be used to describe both the tooth crown surfaces and directions of tooth movement (maxillary left central incisor tooth is depicted).
Mesial: This term means towards the dental midline, along the dental arch.
Distal: This term means away from the dental midline, along the dental arch.
Buccal (labial): The term ‘buccal’ means in the direction of the cheeks; it is ideally used for the posterior teeth but may be used as an inclusive term for both posterior and anterior teeth. The terms ‘labial’ or ‘facial’ mean in the direction of the lips; they are only used for the incisor teeth.
Lingual (palatal): The term ‘lingual’ means in the direction of the tongue; it also refers to the tooth surface facing the tongue. The term ‘palatal’ may be used when referring to the maxillary dentition.
Apical: This term means towards the root apex.
Occlusal (incisal): The term ‘occlusal’ means in the direction of the masticatory surfaces of the teeth. The term ‘incisal’ is the equivalent for the incisor teeth.
Terms of tooth position in the three planes of space
The term bodily displacement refers to the malposition of the crown and root of a tooth in the same direction and to a similar extent. The terms presented below may be used to describe tooth position and/or malposition in the three planes of space:
Sagittal (anteroposterior) plane: Variations in the position of individual teeth in the sagittal plane may be termed labial/buccal or lingual/palatal bodily displacement.
Vertical plane: Variations in the position of individual teeth in the vertical plane may be termed infraocclusion (excessively apically positioned) and supraeruption or overeruption (excessively occlusally positioned).
Transverse plane: Variations in the position of incisor teeth in the transverse plane may be termed mesial or distal bodily displacement. Variations in the position of individual posterior teeth in the transverse plane may be termed buccal or lingual/palatal bodily displacement.
Terms of bodily tooth movement in the three planes of space
The term translation may be defined as the movement of a body from one point of space to another such that every point of the body moves in the same direction and over the same distance, without any form of rotation or change in size. In dental nomenclature, the term translation is synonymous with bodily tooth movement. The following terms may be used to describe bodily tooth movement in the three planes of space:
Sagittal (anteroposterior) plane: Bodily tooth movement (translation) in the labiolingual direction for incisor teeth and the mesiodistal direction for the buccal segments may be termed protraction (labial incisor movement or mesial buccal segment movement) and retraction (lingual/palatal incisor movement or distal buccal segment movement).
Vertical plane: Bodily tooth movement (translation) in the occlusal‐apical direction may be termed intrusion (apical movement) and extrusion (occlusal/incisal movement).
Transverse plane: Bodily incisor movement (translation) in the mesiodistal direction may be termed mesial or distal bodily movement. Bodily movement of individual posterior teeth in the buccolingual direction may be termed buccal or lingual/palatal bodily movement.
Terms of tooth rotation around the three axes of rotation
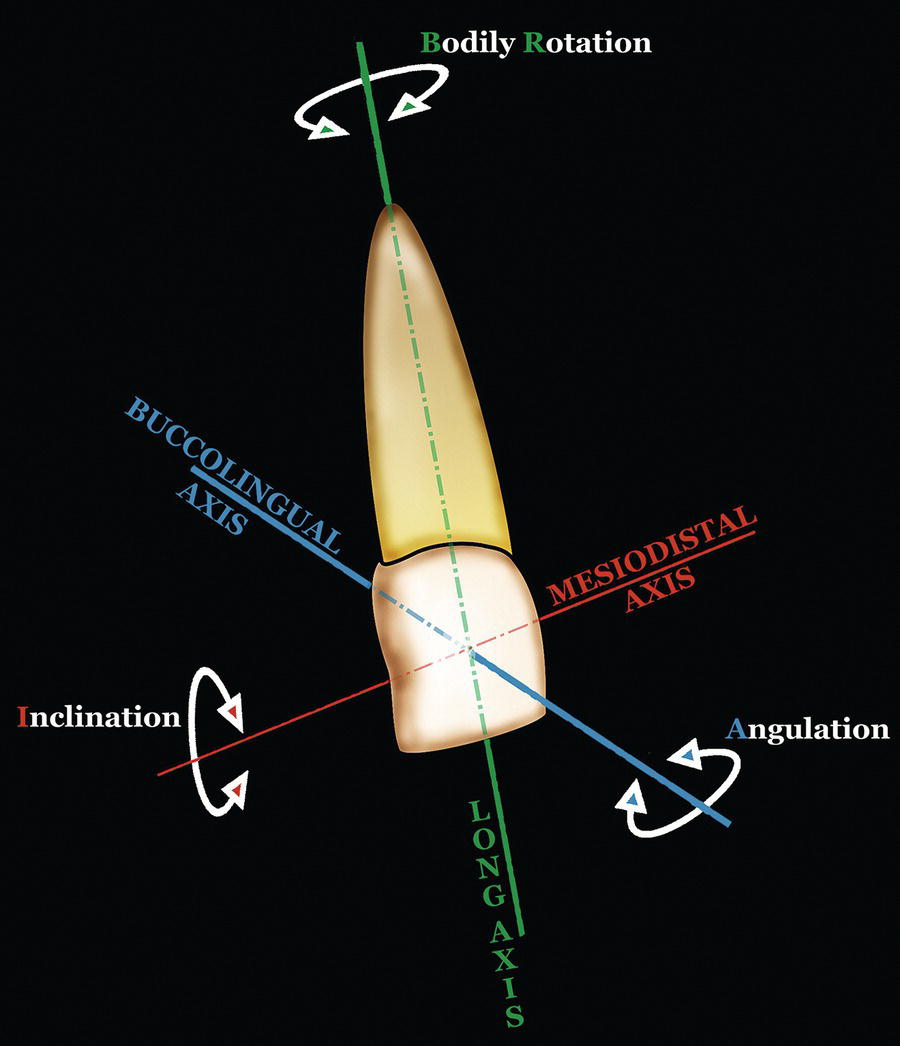
The terminology used to describe the structural relationship of the teeth in relation to the three axes of rotation (Figure 22.2) is as follows:
Angulation: This term refers to the angular deviation of the long axis of a tooth from a line perpendicular to the occlusal plane, in the mesiodistal direction. Rotation of an incisor tooth around the sagittal (labiolingual/buccolingual) axis (also termed second‐order rotation) leads to a change in its angulation.
Inclination: This term refers to the angular deviation of the long axis of a tooth from a line perpendicular to the occlusal plane, in the labiolingual or buccolingual direction. Rotation of a tooth around the mesiodistal (transverse/horizontal) axis (also termed third‐order rotation) leads to a change in its inclination.
Figure 22.2 Terms of tooth rotation around the three axes of rotation.
Proclination: refers to anterior (labial) inclination of the crowns of the incisor teeth.
Retroclination: refers to lingual/palatal inclination of the crowns of the incisor teeth.
Bodily rotation: This term refers to the rotation of a tooth around its long (occlusal‐apical) axis. It is also termed first‐order rotation. Rotations are described according to the approximal surface of the tooth that is furthest from the line of the arch, e.g. a maxillary incisor may be mesio‐ or distolabially rotated or mesio‐ or distopalatally rotated.
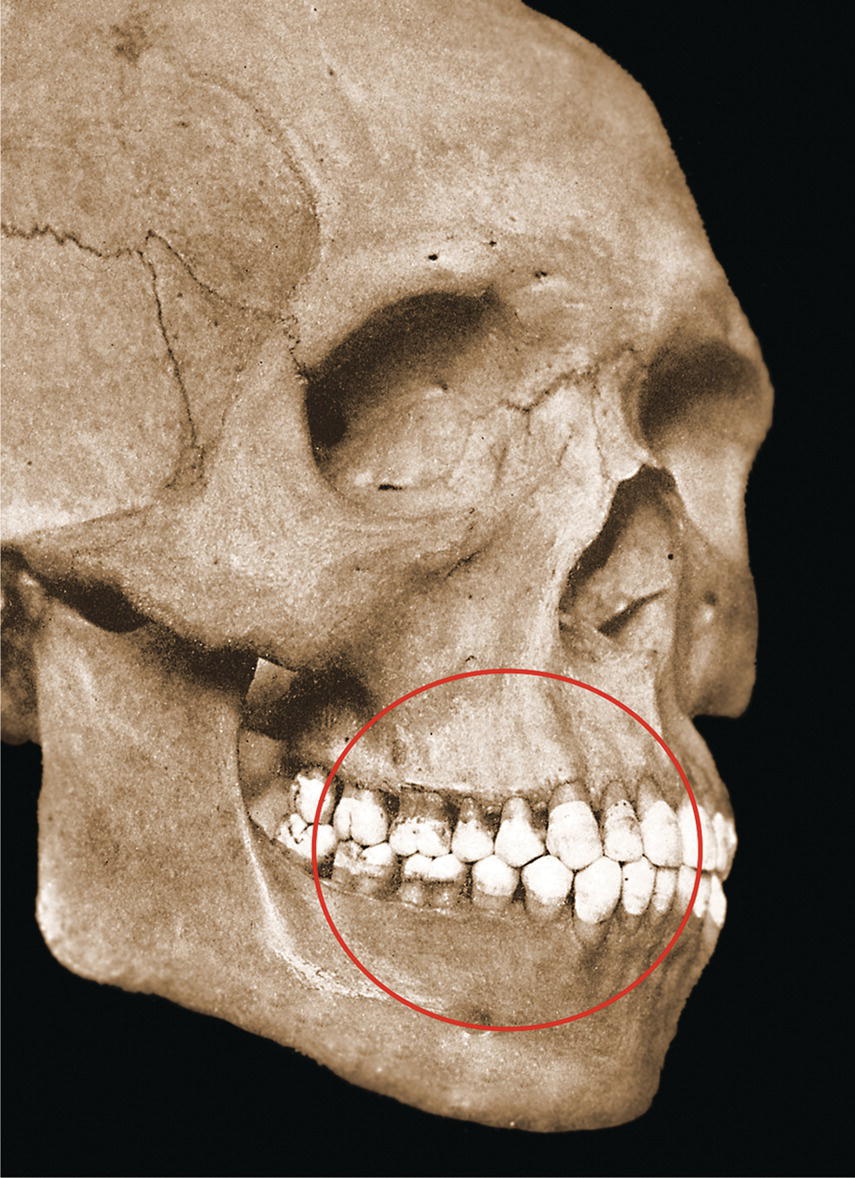
Figure 22.3 The skull named ‘Old Glory’ was used by Edward Angle to exemplify ‘normal’ dental occlusion, though it was the ‘ideal’ to which orthodontists were taught to strive. An element of bimaxillary dentoalveolar protrusion is evident, which does not fit the ‘straight’ facial profile concept, also described by Angle.
The term dental occlusion describes the relationship of the maxillary and mandibular teeth as they are brought into functional contact. The etymology is from the Latin occludere, meaning ‘to close up’. In laypeople’s terms, the occlusion is the ‘bite’ of the teeth. The term ‘ideal’ occlusion is a theoretical concept based on the morphology of unworn teeth of ‘ideal’ size in an ‘ideal’ arrangement; it is almost never found in nature (Figure 22.3).1 The significance of the concept of ‘ideal’ occlusion is as the theoretical standard to which other occlusions may be compared.2
In contrast, the term ‘normal’ occlusion has no precise definition and defies accurate description; normal occlusion is dental occlusion that allows for minor variations from the ‘ideal,’ which are functionally and aesthetically satisfactory. More severe variations, whether in tooth position or arch relationship, are described as malocclusion.3 There is no precise boundary between normal occlusion and malocclusion.
Curves of the occlusion
Sagittal curve of occlusion
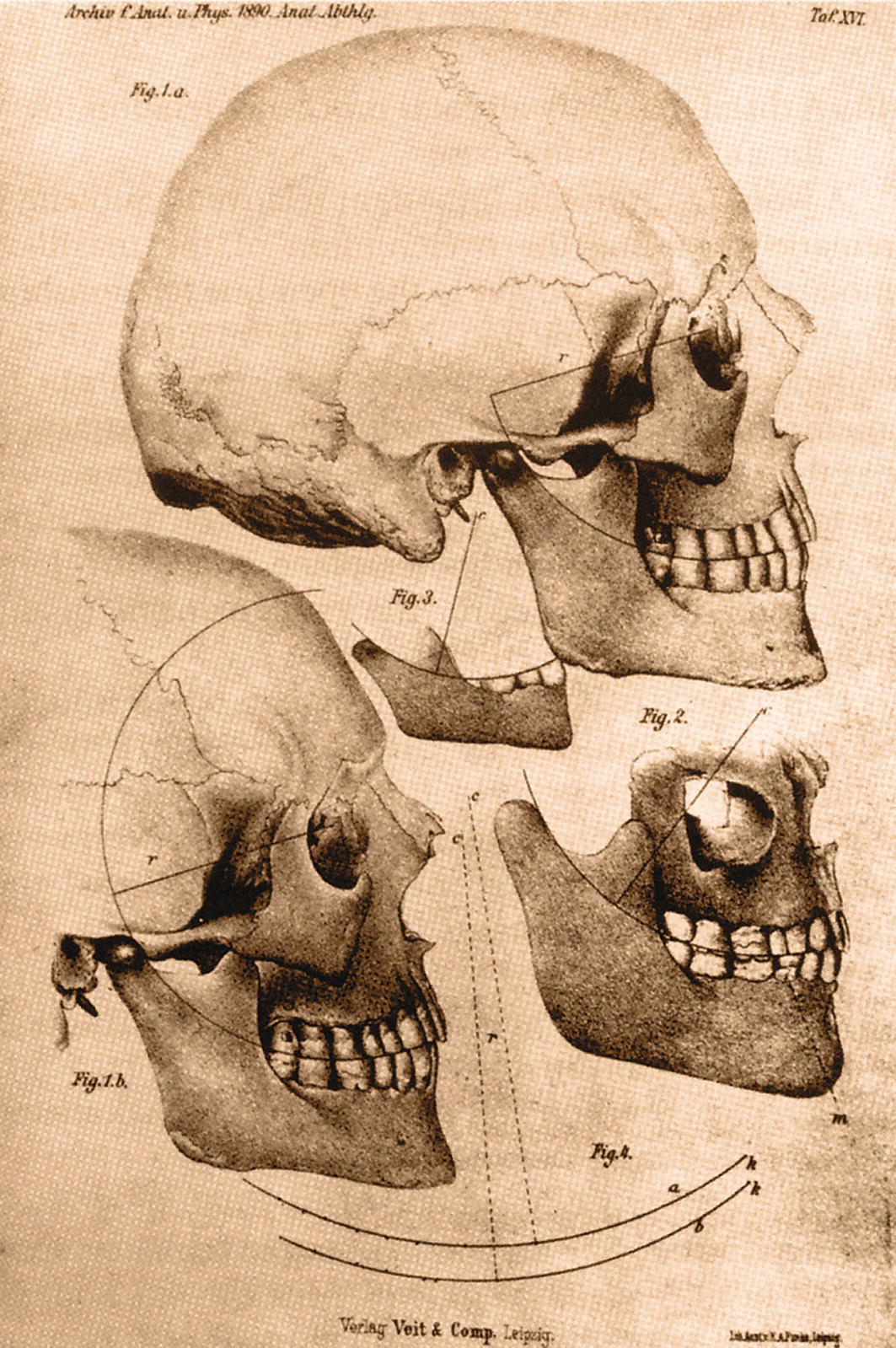
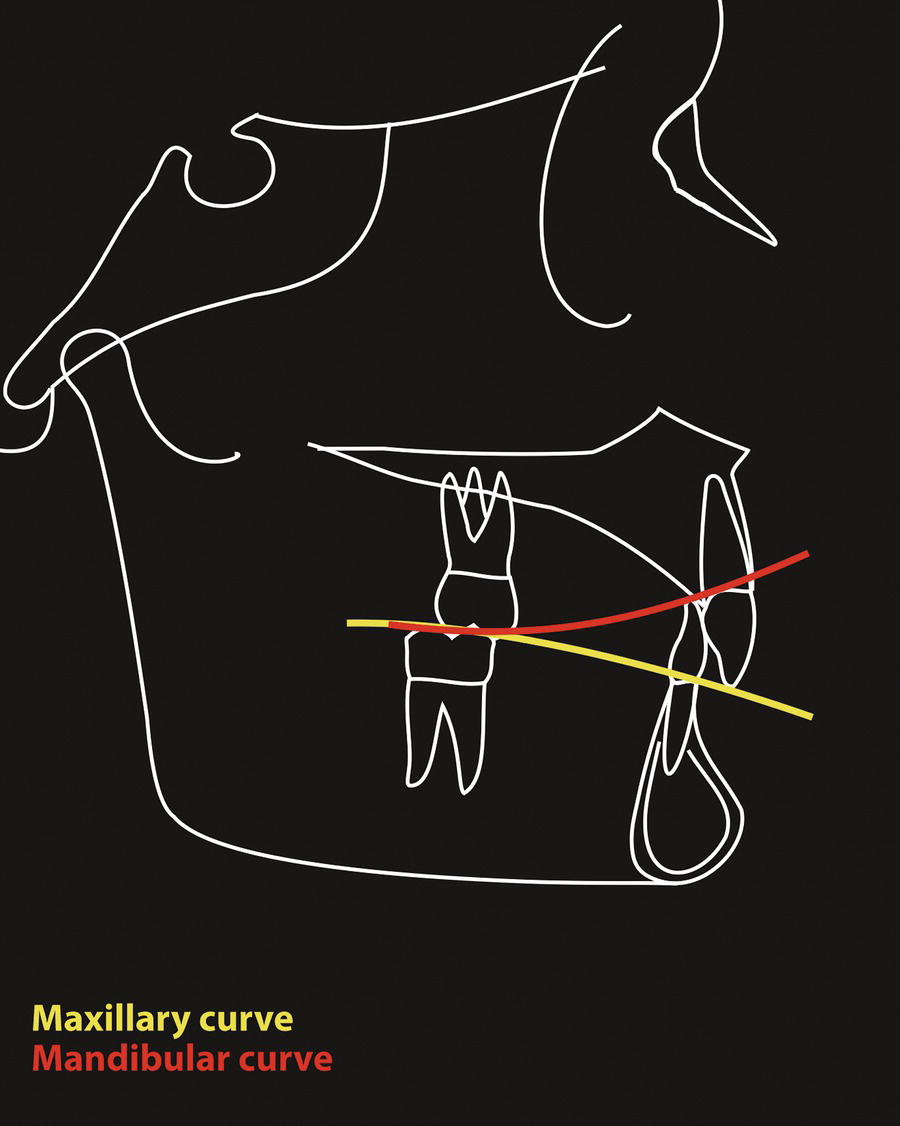
In a normal occlusion viewed from the lateral, the teeth are positioned in such a way that they follow a sagittal curve, with the mandibular cusps becoming more superiorly positioned progressively distally and the maxillary cusps following suit. In the mandibular arch this sagittal curve is termed the curve of Spee, after its description by the German anatomist Ferdinand Graf von Spee (1890).4 In the maxillary arch it is correctly termed the sagittal curve of occlusion, though the term ‘curve of Spee’ is often used to refer to both the mandibular and maxillary curves. Spee originally described the curve with its axis located in the region of the lacrimal bone, with a radius of 65–70 mm in adults.5 The curve was described as contacting the mandibular incisal edge, first molar mesiobuccal cusp, third molar distobuccal cusp and extending to the anterior surface of the mandibular condyle (Figure 22.4).
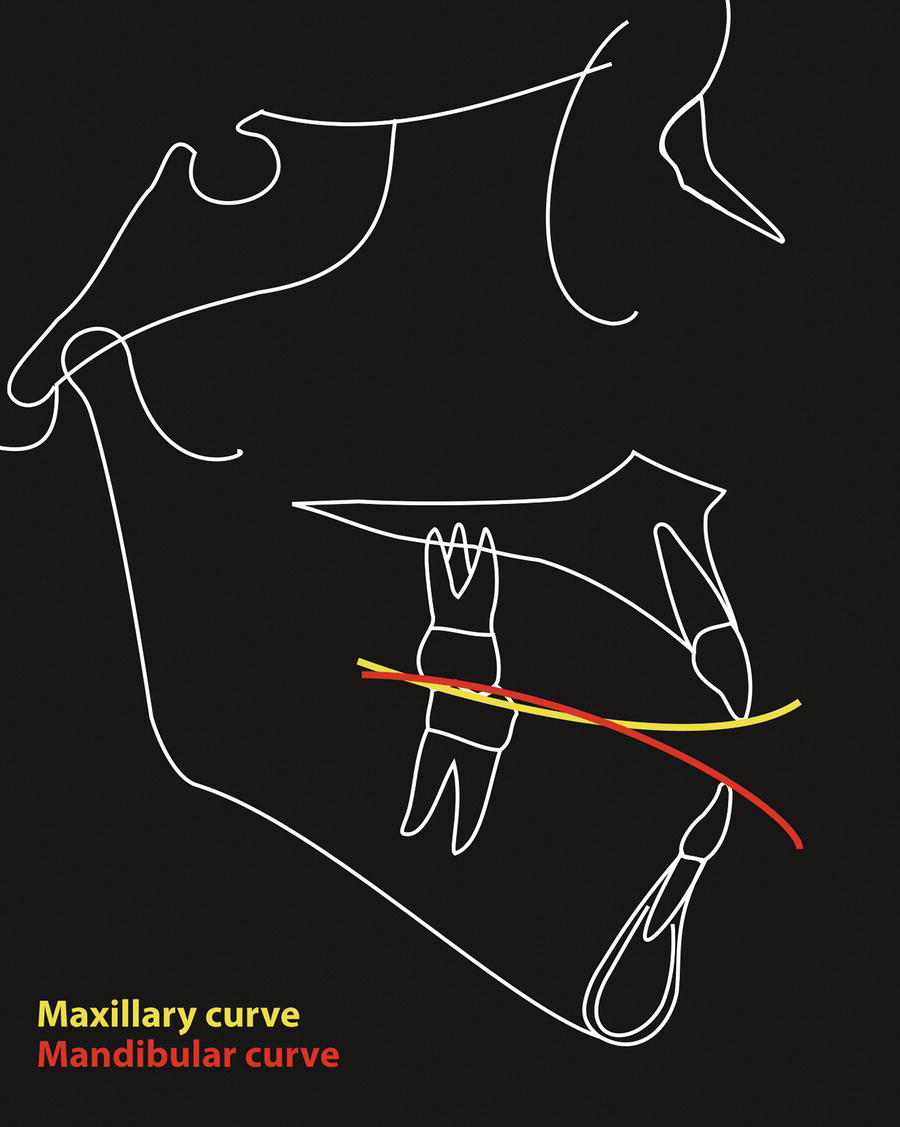
This sagittal curve of occlusion may be accentuated, e.g. if the mandibular incisors are overerupted or the maxillary incisors are unable to fully erupt, or reversed, e.g. if the mandibular incisors have been unable to fully erupt as a result of a forward tongue position in a patient with a soft tissue anterior open bite, or if the maxillary incisors are overerupted. The sagittal curve of occlusion should be described separately for the maxillary and mandibular arches.
Figure 22.4 The ‘curve of Spee’ or sagittal curve of the occlusion
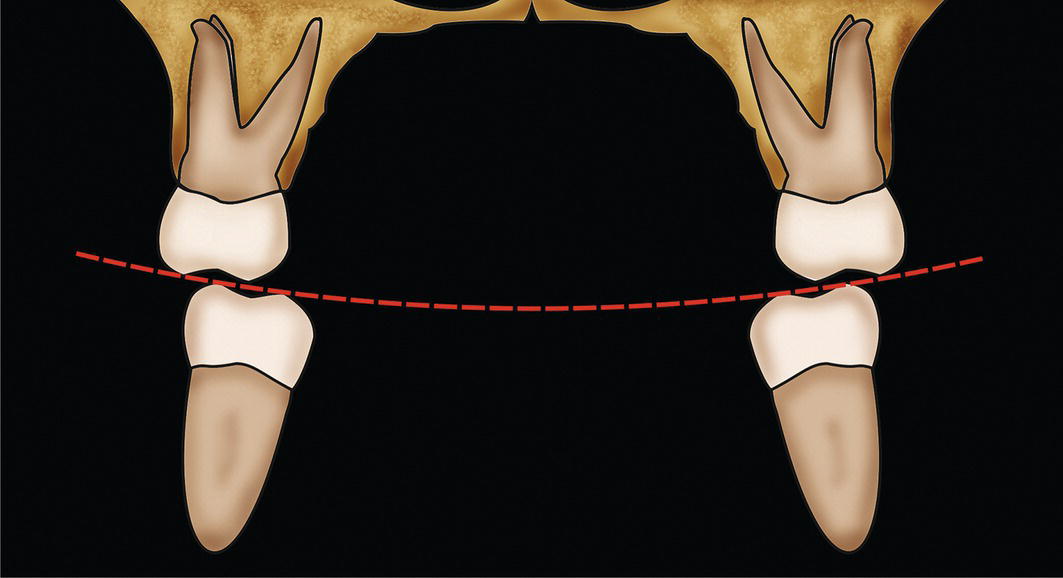
In a normal occlusion viewed from the front, the mandibular posterior teeth are inclined lingually in such a way that the buccal cusps of the mandibular posterior teeth are slightly higher than the lingual cusps; this forms what is termed the curve of Wilson, described by the American dentist George H Wilson in 1911.6 It is alternatively termed the mediolateral curve of occlusion (Figure 22.7).
Aims of treatment and the ‘six keys’ to ‘ideal’ occlusion
It is important to have clear, objective aims before commencing treatment. The orthodontist Lawrence F Andrews (1972) analysed the morphological characteristics of 120 dental study models of untreated individuals with excellent dental occlusions; he studied the tooth crowns in this collection, in order to ascertain the characteristics found consistently in all the models.7 Andrews thereby described these required elements as the ‘six keys to normal occlusion’, though it is apparent that the description relates to an ‘ideal’ rather than a ‘normal’ occlusion (Figure 22.8).
Figure 22.5 Sagittal occlusal curves: the maxillary and mandibular incisors have overerupted past each other, creating a reverse curve in the maxillary arch and an accentuated curve of Spee in the mandibular arch.
Figure 22.6 Sagittal occlusal curves: the maxillary and mandibular incisors have been prevented from erupting to their full potential by a forward resting tongue position, leading to an accentuated curve in the maxillary arch and a reverse curve in the mandibular arch.
Figure 22.7 The transverse curve of occlusion is termed the ‘curve of Wilson’ or the mediolateral curve of occlusion.
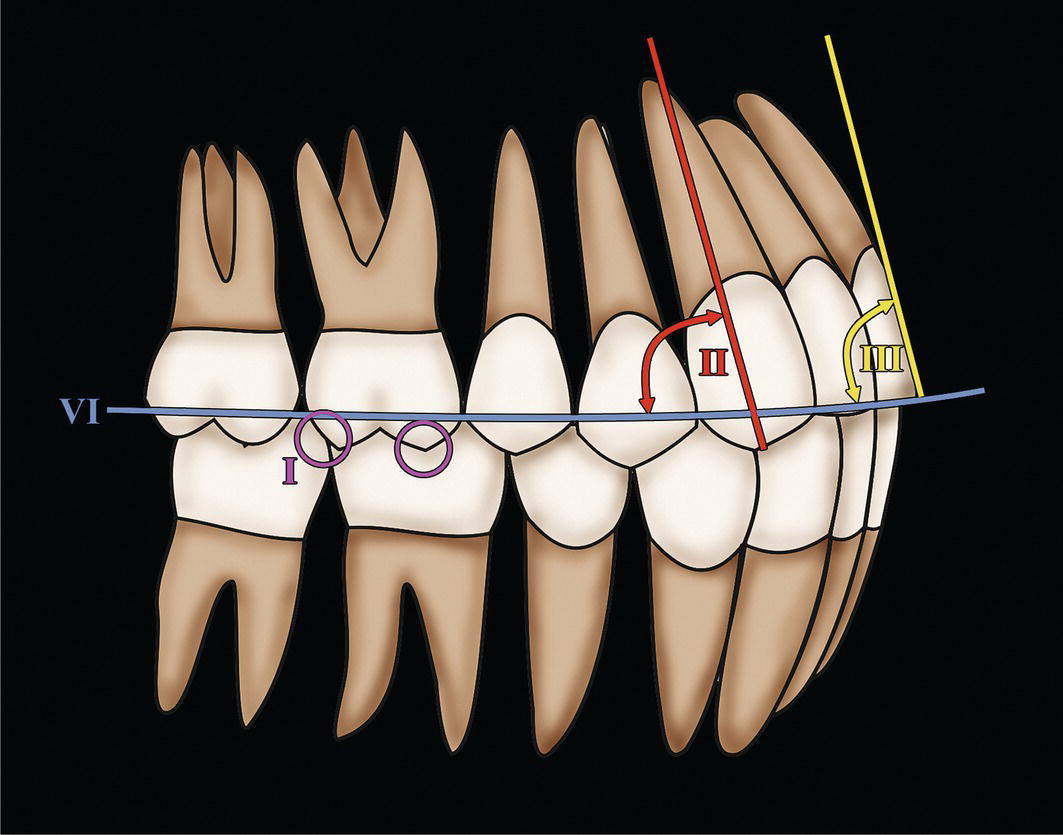
Figure 22.8 Andrews’ ‘six keys’ to ‘ideal’ dental occlusion:
Key I: molar relationship
Key II: crown angulation (mesiodistal angulation)
Key III: crown inclination (buccolingual)
Key IV: no rotations (not shown)
Key V: no interdental spaces (not shown)
Key VI: almost flat curve of Spee.
Key I – Molar relationship: The distal surface of the distobuccal cusp of the maxillary first permanent molar occludes (makes contact) with the mesial surface of the mesiobuccal cusp of the mandibular second permanent molar. The mesiobuccal cusp of the maxillary first permanent molar falls within the buccal groove between the mesial and middle cusps of the mandibular first permanent molar. (The canines and premolars exhibit a cusp‐to‐embrasure relationship buccally and a cusp‐to‐fossa relationship lingually.)
Key II – Crown angulation: This key considers the mesiodistal angulation of the long axis of the clinical crown of each tooth, rather than the long axis of the entire tooth. The gingival portion of the long axis of each crown is distal to the occlusal (incisal) portion; the degree of mesiodistal crown angulation varies for each tooth type. (The long axis of the crown for all teeth, except molars, is judged by the mid‐developmental ridge, which is the most prominent and centremost vertical portion of the labial/buccal surface of the crown. The long axis of the molar crown is identified by the dominant vertical groove on the buccal surface of the crown.)
Key III – Crown inclination: Crown inclination refers to the labiolingual or buccolingual inclination of the long axis of the crown, not to the inclination of the long axis of the entire tooth. The inclination of all the crowns has a consistent scheme:
Incisor teeth: Maxillary and mandibular incisor crowns are labially inclined to a degree sufficient to resist overeruption of their antagonists. The labial inclination permits proper distal positioning of the contact points of the maxillary teeth in relation to the respective contact points of the mandibular antagonists, allowing proper occlusion of the posterior crowns.
Maxillary posterior teeth (canines to molars): A palatal (lingual) crown inclination exists, which is relatively constant from the canines through to the second premolars and is slightly more pronounced in the molars.
Mandibular posterior teeth (canines to molars): The crowns of the mandibular posterior teeth exhibit a lingual inclination that increases progressively from the canines through to the second molars.
Key IV – Rotations: No rotations are present.
Key V – Spaces: There are no spaces; interdental contact points are tight.
Key VI – Occlusal plane: The sagittal plane of occlusion varies from flat to a slight curve of Spee.
Correct tooth size: the ‘seventh key’ to ‘ideal’ occlusion
Bennett and McLaughlin8 described an additional key (seventh key) required for an ‘ideal’ or normal dental‐occlusal relationship: correct tooth size. The presence of a tooth size discrepancy between the maxillary and mandibular dental arches would otherwise result in either crowding or spacing, or compensatory angulations or inclination of the anterior teeth (Figure 22.9).
Only gold members can continue reading. Log In or Register to continue
Nov 8, 2025 | Posted by admin in Aesthetic plastic surgery | Comments Off on Dental‐Occlusal Relationships: Terminology, Description and Classification