, Jane Tomimori1, Sofia Beatriz Machado de Mendonça1 and Douglas Antonio Rodrigues1
(1)
Universidade Federal de São Paulo, São Paulo, Brazil
6.1 Seborrheic Keratosis
Seborrheic keratosis is a common benign proliferation of epidermal cells . This dermatosis can occur in any skin phototype; however, the pigmented form is more frequent in high skin phototypes.
There is no predilection for sex, and older populations (over 40 years) are affected. Lesions develop with progression in size and number. Sun exposure and age are implicated factors.
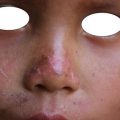
The clinical presentation consists of keratotic and waxy papules and plaques with horn pseudocysts. A papillomatous or verrucous surface is very common, and its colors range from rose to brown-black (Fig. 6.1) . The papules and plaques mainly affect the face and trunk, although isolated lesions may develop on extremities. There is a flat macular form that occurs mainly on the face, which can be mistaken for solar melanosis.

Fig. 6.1
Seborrheic keratosis: single keratotic lesion on face
Diagnosis is clinical; however, histopathology is quite characteristic with hyperkeratosis and proliferation of squamous and basaloid cells. The presence of horn pseudocysts is characteristic. Lesions are treated by chemical cauterization (trichloroacetic acid), electrodessication, and cryotherapy (liquid nitrogen). Surgical shave excision is another possibility. Like the Asian population, the indigenous population presents the pigmented macular form. During their evolution, these lesions become verrucous or papillomatous.
6.2 Melanocytic Nevi
Melanocytic nevi are derived from modified melanocytes (cells responsible for skin color ). They can be congenital (present from birth) or acquired (arise over the course of one’s life). They are related to genetic and environmental factors (exposure to sunlight, in the case of acquired nevi) and are commonly called signs or speckles .
The epidemiological importance of nevi is associated with some risk of transformation into a type of skin cancer called cutaneous melanoma , but the assessment of this risk takes into account many factors that should be analyzed for each situation (such as skin type, age, family history of melanoma). Melanocitic nevi are well circumscribed, brownish or blackish colored, and round or ovoid in shape. They may range in size from a few millimeters to several centimeters (Figs. 6.2, 6.3, 6.4, and 6.5) .




Fig. 6.2
Melanocytic nevi: lesions on face
Fig. 6.3
Melanocytic nevi: lesion on face
Fig. 6.4
Melanocytic nevi: lesions on chest
Fig. 6.5
Melanocytic nevi – lesions on the face
Clinical signs requiring the attention of health professionals are asymmetry, irregular edges, many different colors in the same lesion, a size greater than 6 mm, and rapid growth. These indicate the initial changes into atypical nevi or melanoma. When there is a suspicion that a nevus is atypical, a biopsy of the patient’s lesion should be taken for pathological examination. In most cases no treatment is necessary, only clinical follow-up. When there is suspicion of transformation to melanoma, excisional biopsy is indicated. Among indigenous populations , special attention is required for acral lentiginous melanoma and atypical nevi on the soles and palms. In spite of intense exposure to the sun without sunscreen protection, there have been no reports of melanoma in Xingu Indigenous Park, showing that genetic factors are very important for melanoma onset.
6.3 Nevus Depigmentosus
Nevus depigmentosus is a congenital cutaneous condition characterized by irregularly shaped hypopigmented spots of varying sizes and well-defined borders (Figs. 6.6). They can be located at or follow the lines of Blaschko . The condition may be less evident at birth and better visualized later. Most of the time it appears in the first 3 years of life. Examination under Wood’s light will reveal the spots .

Fig. 6.6
Nevus depigmentosus: lesions on dorsum
Nevus depigmentosus is usually an isolated condition of the skin but may be related to other changes (neurological, orthopedic). Differential diagnosis should be made with vitiligo and nevus anemicus. In countries where leprosy is endemic, a differential diagnosis should be made with indeterminate leprosy, and a thermal, pain, and tactile sensibility test should be performed. A skin biopsy for anatomopathological examination may be performed if necessary. There will be a decrease in melanin, but there is usually no decrease in the number of melanocytes.
Therapeutic options (laser therapy or melanocyte transplantation) can be indicated if aesthetic impairment is very significant.
6.4 Mucous Cyst
A mucous cyst of the oral mucosa is also called a mucocele . It occurs through damage to minor salivary ducts, resulting in mucoid secretion accumulation in the oral mucosa. Mucoceles are seen more frequently on lower labial mucosa, but they also appear on the floor of the mouth and tongue. There is no preference for age or sex.
A mucous cyst is a dome-shaped, soft, and translucent papule or nodule, usually located on the lower lip mucosa (Fig. 6.7). They can range in size from several millimeters to over 1 cm. When the cyst disrupts, a transparent and viscous liquid (sialomucin) is eliminated.