, Teresa S. Wright2, Crystal Y. Pourciau3 and Bruce R. Smoller4
(1)
Department of Pathology & Immunology, Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas, USA
(2)
Departments of Dermatology and Pediatrics, University of Tennessee Health Science Center, Memphis, TN, USA
(3)
Departments of Dermatology and Pediatrics, Baylor College of Medicine and Texas Children’s Hospital, Houston, Texas, USA
(4)
Department of Pathology and Laboratory Medicine, University of Rochester School of Medicine and Dentistry, Rochester, NY, USA
30.1 Clinical Features
A wide range of cutaneous manifestations has been reported in systemic malignancies of children. Childhood malignancies that are more likely to involve the skin include leukemias, lymphomas, neuroblastoma, sarcomas, and Langerhans cell histiocytosis [1]. Cutaneous lesions of leukemias are highly variable and may include erythematous to violaceous papules, nodules, and plaques on the face, trunk, and extremities (see also Chap. 22). Skin lesions of lymphomas are most common in the head and neck, followed by the abdomen. Solitary or multiple erythematous papules, nodules, and plaques may occur. Lesions may be painful and prone to ulceration. Typical skin lesions of neuroblastoma are firm, blue to purple papules and nodules with a “blueberry muffin” appearance. In children, sarcomas are most likely to involve the head and neck, followed by the genitourinary tract and extremities. Skin lesions are typically asymptomatic solitary soft tissue masses. Therapy is generally aimed at treatment of the underlying malignancy.
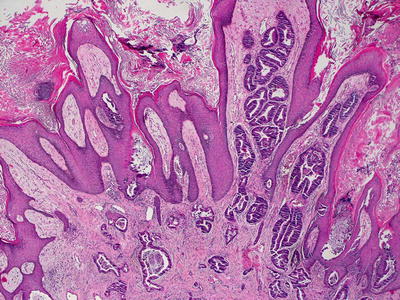
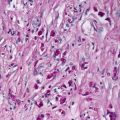
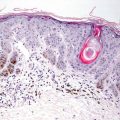
30.2 Histology
The prevalence of cutaneous metastases in children is markedly different than that seen in adults, and it is largely a reflection of the types of neoplasms in children. Neuroblastomas , leukemias , and lymphomas are the neoplastic processes most likely to be encountered in children with histologic features that resemble the primary tumors [2]. As many as one third of patients with neuroblastomas will have cutaneous metastases at some point in the course of their disease progression [3]. Lymph node-based lymphomas can spread to involve the skin. In these cases, it is important to search for systemic involvement before determining that a malignant cutaneous lymphoid infiltrate arose within the skin [4].
Tumors such as medulloblastoma, embryonal and alveolar rhabdomyosarcoma, and choriocarcinoma develop cutaneous metastases much more commonly in children, as these neoplasms are quite rare in adults [5, 6].
Diagnostic work-up of metastatic lesions frequently requires the use of immunostains selected to highlight various specific lines of cellular differentiation of the tumor. A detailed description of all possible visceral malignancies with potential for cutaneous metastasis is beyond the scope of this volume, but knowledge of pediatric tumor pathology is essential in order to fully recognize the full range of diagnostic possibilities. Several examples of cutaneous metastases are seen in the accompanying figures, and demonstrate the characteristic histologic features (Figs. 30.1, 30.2, 30.3, 30.4, 30.5, and 30.6).