CHAPTER 11 Correction of Crossover Toe Deformity
SURGICAL APPROACH
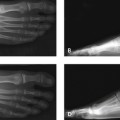
If the crossover deformity is associated with a long second metatarsal, then the second metatarsal should be shortened. Shortening the metatarsal relieves the medial joint contracture because pressure is taken off the intrinsic tendons, as illustrated in Figure 11-1. In this case, the patient presented for treatment 1 year after bilateral hallux valgus correction. An interesting observation is that recurrent hallux valgus did not develop, despite the lack of anatomic barriers to valgus drift of the hallux (see Figure 11-1, A and B). The lesser toe deformities were treated with shortening osteotomies of the lesser metatarsals. The alignment initially was not ideal but improved somewhat with taping of the toes into varus for 3 months after surgery (see Figure 11-1, C).

Treating a crossover toe deformity as a claw toe will lead to prompt recurrence of deformity (Figure 11-2). Repair of the ruptured lateral collateral ligament and volar plate is technically difficult and probably unrealistic. For the repair to be performed, the suture must be inserted into the lateral collateral ligament without restraint of the joint and creation of a dorsiflexion contracture. To approach the plantar aspect of the MP joint with a transverse or longitudinal incision is very difficult, because the plantar joint does not correspond with the plantar skin crease. Techniques for repair of the lateral collateral ligament have been described; an important consideration in the surgical evaluation, however, is the underlying cause of the ligament rupture. If the rupture is the result of wear against the base of the third toe phalanx or from a long metatarsal, will a simple repair correct the deformity? This outcome is very unlikely, and an attempt at an anatomic repair, versus a simpler procedure such as a tendon transfer or a shortening of the metatarsal head, is not worth the effort. In elderly patients, when the MP joint is severely subluxated, with crossover of the toe on the hallux and asymptomatic hallux valgus, amputation of the toe may be a very reasonable option. The hallux does not drift further, because it typically is abutting the third toe already, and the removal of the painful second toe generally is a very successful procedure for the patient (Figure 11-3).


COMPONENTS OF SURGICAL CORRECTION
Extensor Digitorum Brevis Tendon Transfer
If the instability of the toe is predominantly in the transverse and not the sagittal plane, then the extensor digitorum brevis (EDB) tendon transfer, rather than a flexor-to-extensor tendon transfer, is preferred. The EDB tendon and the extensor digitorum longus tendon are identified proximally and dissected free of each other by means of a longitudinal split of the extensor hood with Metzenbaum scissors, as shown in Figure 11-4. In this case, after the proximal interphalangeal (PIP) arthroplasty, the toe is seen sticking up in the air and crossing over the hallux—a classic example of why some decompression of the MP joint is necessary. Some increase in the strength of plantar flexion of the toe is necessary using either a flexor-to-extensor tendon transfer or an extensor brevis tendon transfer. A 6-cm length of the EDB tendon is selected, and before division of the tendon, two nonabsorbable 4-0 sutures are inserted on either side of the tenotomy to stabilize the tendon after its division for transfer. A tenotomy is now performed in between these two sutures, and the distal portion of the EDB tendon is now gradually mobilized. It is dissected free more distally from the extensor hood. Its attachment to the extensor hood overlying the base of the proximal phalanx must be maintained (see Figure 11-4).

If the EDB tendon tears or looks as if it will separate from the extensor hood, then a stay suture can be inserted between the distal tendon and the extensor hood. With the work now being done in the lateral web space, a curved, blunt-tipped (aneurysm) needle is passed from proximal to distal and below the deep transverse metatarsal ligament. The needle is then curved up into the soft tissue, and the suture attached to the EDB tendon is passed through the needle, which is then delivered proximally. The EDB tendon is now pulled deep to the soft tissue tether and passed proximally. As the tendon is pulled, the toe should assume a normal alignment, with good correction in both the transverse and the sagittal planes. Because of the axis of the tendon transfer, the toe may supinate slightly, and this supination must be noted (see Figure 11-4).





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


