Chapter 11 Correction of Alar Rim Deformities
 Animations
AnimationsPearls
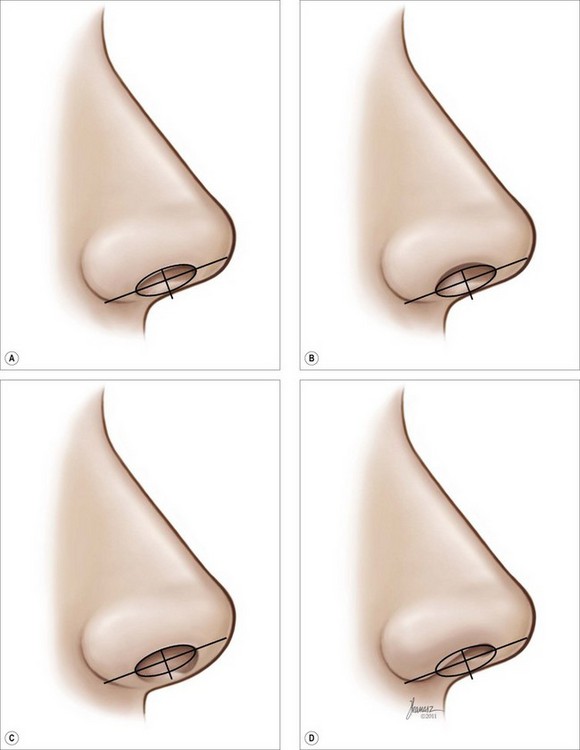
• The optimal ala–columella relationship on the profile requires a symmetric oval outline of the nostril in conjunction with the columellar base that is bisected by the line connecting the most anterior and posterior ends of the nostril.
• Ideally, there is 3–4 mm columellar show caudal to the alar rim. Increased distance cephalad to the bisection line is an indication of an alar retraction, while an increase caudally is a reflection of columella protrusion. A decrease in this distance caudally is an indication of columella retraction, and a decreased distance cephalically may denote a hanging ala.
• Concavity of the ala may exist as a result of natural weakness, over-resection of the lower lateral cartilage, or cephalic malpositioning of the lower lateral cartilages.
• A lateral crura spanning suture, a transdomal suture, or a combination of these can also result in a concave ala.
• To correct the hanging ala, an ellipse is designed within the vestibular lining. The lining and the underlying fibrofatty tissues are excised, and fast absorbable 6-0 catgut is used to repair the defect.
• Alar thickness can be reduced by removing an elliptical piece of soft tissue as far medially along the caudal border of the alar rim as possible.
• Alar convexity can be effectively corrected with a transdomal suture, lateral crura spanning suture, or lateral crura convexity control suture.
• Mild to moderate alar rim retraction can be corrected by placement of an alar rim graft.
• An effective means of correcting alar retraction is a V-Y advancement of the alar lining along with placement of an alar rim graft.
• It is commonly necessary to add internal and external splints to eliminate the dead space and ensure proper advancement of the alar rim.
Gunter et al introduced a classification of alar rim deformities, which was further amended by the author’s team.1,2 Some of these deformities are only visible on the profile view and some are discernible on the basilar view. The optimal ala–columella relationship on the profile requires a symmetric oval outline of the nostril in conjunction with the columella base that is bisected by the line connecting the most anterior and posterior ends of the nostril. Ideally, there is a maximum of 3–4 mm columellar show caudal to the alar rim, which means that the distance between the bisection line and the alar rim is approximately 1.5–2.0 mm (Figure 11.1A). Increased distance cephalad to the bisection line is an indication of an alar retraction, while an increase caudally is a reflection of columella protrusion (Figure 11.1B). A decrease in this distance caudally is an indication of columella retraction, and a decreased distance cephalically may denote a hanging ala (Figure 11.1C). An increase in the distance caudal to the line denotes a hanging columella. The basilar view (Figure 11.2) of the ideal nose demonstrates an equilateral triangle outline with symmetric positioning of the ala tangential to the limbs of the triangle (Figure 11.2A). Concavity of the ala within the triangle may exist as a result of natural weakness, over-resection of the lower lateral cartilage or cephalically malpositioned lower lateral cartilages. A lateral crura spanning suture, a transdomal suture that is placed cephalad through the cartilages, or a combination of these elements may also produce a concave ala (Figure 11.2B). This deformation of the ala imparts a clover leaf shape to the base of the nose, which is aesthetically very displeasing. Domes that are too wide because of lateral extension of the convex lower lateral cartilages can stretch the nostrils outside the triangle. This type of alar morphology is typical of African-American and Asian noses, in which the nostril wall has a normal thickness but extends beyond the optimal nasal base triangle (Figure 11.2C). Significant reduction of tip projection may also cause such a change. Additionally, excessive thickness of the lateral nasal wall can broaden the basilar outline of the nose beyond the triangle (Figure 11.2D). The notching or retraction of the ala can be classed as minimal, moderate, or severe and each may benefit from a different corrective approach.