26 Complications of temporary fillers
Summary and Key Features
• Soft tissue augmentation with temporary fillers continues to be among the most commonly performed cosmetic procedures
• There are a variety of temporary dermal fillers with an ever-increasing number coming to market. As more fillers become available, it is imperative that the aesthetic physician who injects dermal fillers has proper training in their use and understands the differences between them
• Though generally safe, complications can occur with temporary fillers; physicians need to recognize and manage these complications when they present
• Peri-procedural adverse events such as bruising, swelling, and pain are extremely common and usually resolve in less than 7 days
• Proper injection technique is crucial to minimize visible and / or symptomatic papules and nodules
• To minimize the risk of infection and biofilm formation, one should consider a skin preparation utilizing chlorhexidine and / or isopropyl alcohol
• The cause of granulomatous reaction is multifactorial and may be due to a true foreign-body reaction to the particulate or gelatinous filler or to the emergence of a biofilm
• Early institution of antibiotics, often for a prolonged period, is vital when a patient presents with inflammatory papules and nodules
• Early recognition of impending necrosis after injection is critical; treatment with hyaluronidase, topical nitroglycerin, and massage may be required
• Judicious use of injectables requires an appreciation of normal facial anatomy and the changes that occur with the aging process
• There is an alarming trend of increasing numbers of non-aesthetic physicians and non-MDs using these products; one may expect to see potential complications in the office
Introduction
Materials approved for soft tissue augmentation can be divided into biodegradable, semibiodegradable, and non-biodegradable products. These classifications correlate with their duration of effect as being temporary (approximately 6–12 months), temporary-plus (duration up to 18 months), or permanent (Box 26.1). As more fillers become available, it is imperative to understand the differences between them, the complications that can occur from each, and how best to avoid and treat them when they do occur.



Potential complications associated with temporary soft tissue fillers can be categorized by the time of onset (Box 26.2). In general, adverse events can be subdivided into acute and delayed reactions. Acute reactions are procedural or related to injection technique. They are usually transient and are manifested by erythema, edema, ecchymosis, pruritus, and pain in the first week after injection. Delayed reactions are related to the product itself, or the interaction between the filler and the host response. They are usually manifested by persistent erythema, swelling, nodules, and indurations developing months to years after. The nature of these reactions and their treatment will be summarized in this chapter.








Injection site reactions
The most common adverse events associated with fillers are local injection site reactions, manifested by pain, erythema, and edema. They are typically mild, localized, and transient, resolving within 4–7 days. A recent study by Brandt et al evaluating the efficacy and safety of biphasic hyaluronic acid Restylane® and Perlane® in the lower face revealed that the majority of patients treated with both small and large gel-particle hyaluronic acid experienced at least one injection site reaction. The reported events in decreasing order of occurrence consisted of bruising, tenderness, swelling, and redness. In another study comparing hyaluronic acid (Restylane®) with collagen (Zyplast®) for the treatment of nasolabial folds in contralateral sides, injection site reactions occurred at 93.5% and 90.6% of the hyaluronic acid and collagen treated sites, respectively. The bruising can be severe, especially in patients who have taken antiplatelet agents such as aspirin or non-steroidal anti-inflammatory agents, as shown in Figure 26.1.

Edema and ecchymosis
Some of the most common post-procedure adverse events are bruising and swelling secondary to local trauma from the injection (Fig. 26.1). Reviewing all medications and supplements with the patient can minimize the degree of edema and ecchymosis. Avoidance of agents that inhibit coagulation is recommended, including aspirin (unless taking for ‘therapeutic’ indications) and non-steroidal anti-inflammatory medications, as well as supplements such as garlic and Ginkgo biloba that have an inhibitory effect on platelets. Other supplements such as vitamin E, fish oil, glucosamine, ginger, ginseng, green tea, and celery root can inhibit coagulation pathways and further increase bleeding and bruising. It is recommended to withhold these supplements at least 5 days prior to treatment.
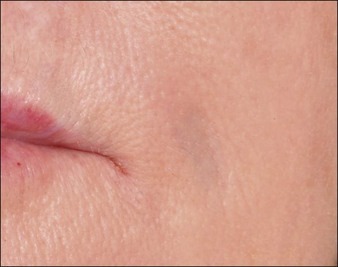
Nodules and papules
Inappropriate placement of fillers may result in the development of subcutaneous nodules and papules. The majority of these are manifested as palpable and / or visible bumps under the skin. Injecting too superficially can lead to lumps of visible product, or bluish bumps under the skin explained by the Tyndall effect with hyaluronic acid fillers (Fig. 26.2). Such reactions can, for the most part, be prevented by use of correct technique. Treatment of visible papules can often be accomplished by firm digital pressure, by aspiration, or by incision and drainage. When persistent papules and nodules are due to the use of a hyaluronic acid filler, the enzyme hyaluronidase can be utilized to treat them.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


