11 Complications and legal considerations of laser and light treatments
General complications
Hyperpigmentation (Fig. 11.1) is a very common complication and possibly the most common in darker skin types (see the study by Sriprachya-anunt and colleagues). It has been described with the use of almost every laser and light device in darker skin types. In one study by Moreno-Arias and co-workers, it was observed in 16% of patients undergoing IPL treatment. Goh reported that it can be as high as 45% in patients with skin types IV–VI. Wareham et al reported that the pulse dye laser can cause hyperpigmentation, especially on the lower legs and where there is inadequate post-treatment sun protection and sun avoidance. Hyperpigmentation was also seen by Chowdhury and colleagues with the KTP laser. With the ablative CO2 laser, post-inflammatory hyperpigmentation (PIH) is common and was reported by Badawi et al to occur in 20–30% of Fitzpatrick III and 100% of Fitzpatrick IV patients. Mahmoud et al found the Er : YAG laser to have a PIH rate of 50% in patients with skin type IV–V (Fig. 11.2). Even non-ablative fractional lasers can cause problems with PIH; in a 2010 study by Chan et al there was an 18.2% rate in 47 patients treated. Although rarer, PIH has also been reported (e.g. by Choudhary et al and Kuperman-Beade et al) to occur with the use of Q-switched lasers. In darker skin types, it can be fairly common; it was reported by Lapidoth & Aharonowitz to occur in up to 44% of darker-skinned patients. As noted above, vascular lasers were also found by Clark et al to result in PIH, albeit more rarely.

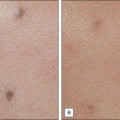
Figure 11.1 Post-inflammatory hyperpigmentation following treatment with the Q-switched Nd : YAG laser.

Scarring has been reported with almost every cutaneous laser and light source (Figs 11.3–11.6). The actual incidence is fairly small, yet overaggressive treatment with any laser or light device can cause it. Hypertrophic scarring is most common with the older continuous wave lasers, most of which are no longer commonly used in office practice.




Specific laser complications
Q-switched lasers
In the study by Kuperman-Beade and co-workers, the most common adverse effects of the Q-switched lasers included hypo- and hyperpigmentation, textural change, and scarring after treatment (see Fig. 11.1). Melanin is the main competing chromophore and transient hypopigmentation as well as permanent depigmentation with the Q-switched ruby laser can be seen (see the study above and those by Bernstein and Choudhary et al). Grevelink et al found that the Q-switched Nd : YAG laser with its longer wavelength has less chance of hypopigmentation than the Q-switched ruby laser. In darker-skinned individuals, if a Q-switched laser other than the Nd : YAG laser is used then decreasing the fluence may help prevent hypopigmentation, according to Kuperman-Beade et al.




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


