(1)
Hôpital Universitaire de Strasbourg, Strasbourg, France
12.1 Acne
12.2 Rosacea
12.4 Atopic Dermatitis
12.6 Urticaria
12.7 Psoriasis
12.10 Scabies
12.11 Dermatophytosis
12.12 Impetigo and Ecthyma
12.13 Pyodermas
12.17 Other Infections
12.18 Scar
Abstract
Comedos, microcysts, red papules, and papulopustules (Figs. 12.1 and 12.2). Lesions are located on the face, particularly the jugal areas and the forehead, as well as the back. The comedo (“black spot” (white arrow)) and the microcyst (black arrow) are the most characteristic primary lesions of acne. The diagnosis of acne cannot be established without the presence of at least one of these two lesions, especially since papules and papulopustules are also present in rosacea, which is another prevalent facial dermatosis (cf. Figs. 12.3 and 12.4).
12.1 Acne
Comedos, microcysts, red papules, and papulopustules (Figs. 12.1 and 12.2). Lesions are located on the face, particularly the jugal areas and the forehead, as well as the back. The comedo (“black spot” (white arrow)) and the microcyst (black arrow) are the most characteristic primary lesions of acne. The diagnosis of acne cannot be established without the presence of at least one of these two lesions, especially since papules and papulopustules are also present in rosacea, which is another prevalent facial dermatosis (cf. Figs. 12.3 and 12.4).


Fig. 12.1
∎
Fig. 12.2
∎
12.2 Rosacea
Midfacial erythema with telangiectasia, which spares the “mobile” areas of the face such as the eyelids and the circumoral area (Fig. 12.3). Papules, pustules, and papulopustules can appear on the facial erythema (Fig. 12.4). Comedos and microcysts are absent, as opposed to acne (cf. Figs. 12.1 and 12.2).


Fig. 12.3
∎
Fig. 12.4
∎
12.3 Seborrheic Dermatitis
Recurring scaly erythema, predominant in areas rich in sebum: hairline, glabella, nasolabial folds, and presternal area (Figs. 12.5–12.7).
Some patients will have lesions characteristic of both seborrheic dermatitis and rosacea at the same time (Fig. 12.8): This entity is known in the French nosology under the designation of mixed dermatitis of the face.




Fig. 12.5
∎
Fig. 12.6
∎
Fig. 12.7
∎
Fig. 12.8
∎
12.4 Atopic Dermatitis
Erythema of the cheeks and more generally of convex areas, in infants under 6 months (Fig. 12.9). Scaly erythema of the folds, more or less lichenified and excoriated, in adults and infants older than 6 months (Fig. 12.10). The skin is usually dry (xerosis) and the accentuation of the inferior palpebral folds is typical (Dennie-Morgan sign: double inferior palpebral fold (arrow), Fig. 12.11). Herpetic superinfection is frequent. It can be localized (Fig. 12.12; note the grouped and dried vesicles) or sometimes generalized and febrile. In the latter case, it is called the Kaposi-Juliusberg’s syndrome, which is a life-threatening condition.


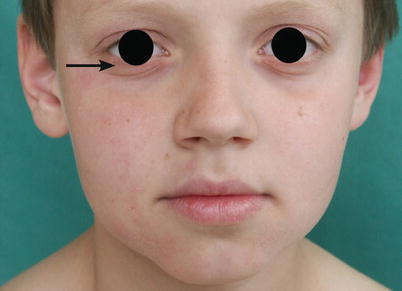

Fig. 12.9
∎
Fig. 12.10
∎
Fig. 12.11
∎
Fig. 12.12
∎
12.5 Allergic Contact Dermatitis (Eczema)
Erosive, oozing, and/or crusting erythema (Figs. 12.13, 12.14, and 12.15). Acute eczema progresses through the following stages: erythema, vesicle, oozing, and crusting. Chronic forms are erythematous, scaly, and dry (Fig. 12.16). There are several variants: bullous (Fig. 12.17), edematous, pustular (cf. Fig. 5.14), etc. Significant pruritus is present in all stages. In contact dermatitis caused by hair dye, the upper part of the face is highly edematous (Fig. 12.18) and can easily be mistaken with angioedema (urticaria of deeper skin tissues, Quincke’s edema).






Fig. 12.13
∎
Fig. 12.14
∎
Fig. 12.15
∎
Fig. 12.16
∎
Fig. 12.17
∎
Fig. 12.18
∎
12.6 Urticaria
Urticaria is a rash of sudden onset consisting of papules and red, edematous plaques (Fig. 12.19), mostly evanescent and pruritic. The latter semiological features are anamnestic elements and allow establishing diagnosis during history taking. In the absence of these features, it can be difficult to distinguish urticaria and maculopapular exanthema. It must be kept in mind that urticaria can be one of the manifestations of a serious anaphylactic reaction. In case of chronic urticaria, lesions can sometimes be reproduced by rubbing the skin with a blunt tip, which induces erythema + edema + pruritus. This is known as dermographism (Fig. 12.20).


Fig. 12.19
∎
Fig. 12.20
∎
12.7 Psoriasis
Well-defined erythematous and scaly plaques (Fig. 12.21), even when confluent (Fig. 12.22). Psoriasis is a very common dermatosis, affecting around 2 % of the population. It comprises of several clinical expressions which will not all be covered in this book. The plaque form illustrated here is the most common. The most initial lesion of common psoriasis is an erythematous macule (Fig. 12.23) which rapidly becomes scaly and infiltrated; in folds, psoriasis usually persists as an erythematous macule (intertrigo, Fig. 12.24). The sharp demarcation of the lesions is characteristic and allows diagnosis even on dark skin, where erythema is difficult to observe (Fig. 12.25).

Fig. 12.21




∎
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
