14 Combinations of Therapy
Introduction
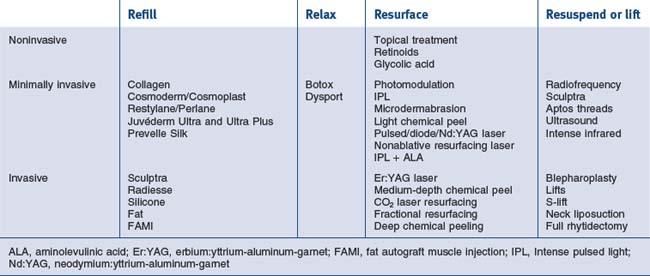
The cosmetic physician’s tools can be divided into the following categories:
The various regenerative procedures are also classified as to the level of aggressiveness and downtime. They range from ‘lunchtime’ procedures and moderately aggressive procedures to fully aggressive procedures. Each of these also can be chosen for the appropriate patient and even the proper unit area of need. These procedures are outlined in Table 14.1. See also Box 14.1.
Box 14.1
Key features
The Analysis of Skin Types
• Fitzpatrick skin type system
The Fitzpatrick skin type system classifies degrees of pigmentation and ability to tan using grades I to VI. It prognosticates sun sensitivity, susceptibility to photodamage and ability for facultative melanogenesis (one’s intrinsic ability to tan). In addition, this system classifies skin as to its risk factors for complications during chemical peeling or other resurfacing procedures. Fitzpatrick skin types take into account both color and reaction to the sun. Skin types I and II are pale white and freckled with a high degree of potential to burn with sun exposure. Types III and IV can burn but usually are an olive to brown coloration. Types V and VI are dark brown to black skin that rarely ever burn and usually do not need sunscreen protection (Table 14.2).
Table 14.2 Fitzpatrick’s classification of skin types
| Skin type | Color | Reaction to sun |
|---|---|---|
| I | Very white or freckled | Always burns |
| II | White | Usually burns |
| III | White to olive | Sometimes burns |
| IV | Brown | Rarely burns |
| V | Dark brown | Very rarely burns |
| VI | Black | Never burns |
• Glogau system
The Glogau system classifies severity of photodamage, taking into account the degree of epidermal and dermal degenerative effects. The categorization is from I to IV, ranging from mild, through moderate and advanced, to severe photodamaged skin. These categories are devised for therapeutic intervention. Type I in young individuals or minimal degree photodamage should be treated with light chemical peeling and medical treatment. Types II and III would entail medium-depth chemical peeling, while type IV would need those modalities listed plus cosmetic surgical intervention for gravitational changes (Box 14.2). Type III or IV can have combination procedures dependent on the degree of damage in each area.
Box 14.2
Photoaging group – Glogau’s classification
Based on Glogau RG 1994 Chemical peeling and aging skin. Journal of Geriatric Dermatology 2(1):30–35
• Index of photoaging skin
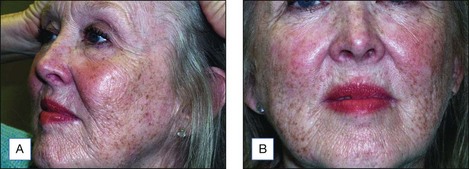
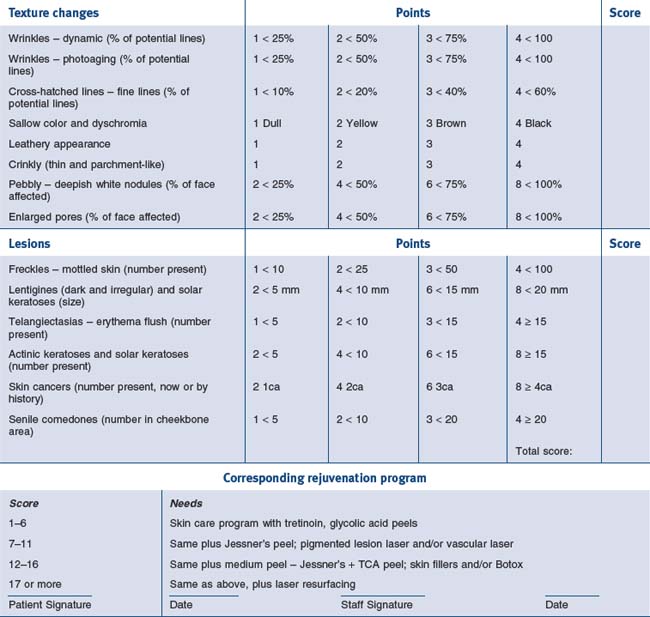
The index of photoaging skin is a system of quantitating photodamage and using numerical scores that would fit into corresponding rejuvenation programs. In analyzing photodamage, the major categories include epidermal color, skin lesions, textural changes, and dermal changes. Photoaging changes include wrinkles, cross-hatched lines, sallow color, leathery appearance, crinkly thin parchment skin, and the pebblish white nodules of milia. Each of these is classified, giving the patient a point score of between one and four. In addition, the number and extent of lesions are categorized from freckles, lentigines, telangiectasias, actinic and seborrheic keratoses, skin cancers, and senile comedones. These are also added in the classification system and the final score results are tabulated. A total score of between one and four indicates very mild damage and the patient would adequately respond to a five-step skin care program including sunscreen protection, retinoic acid, glycolic acid peels and selective lesional removal. A patient scoring between five and nine requires all of the above, plus a repetitive superficial peeling agents program such as glycolic acid, Jessner’s solution or lactic acid peels. A score of 10–14 suggests the inclusion of medium-depth chemical peeling, and if a patient scores 15 or above the practitioner will be including deep peeling or laser resurfacing in the treatment (Figs 14.1 and 14.2). Thus, the patient can understand during the consultation the degree of photodamage and the necessity for an individual peeling program (Table 14.3). The system can also quantitate individual cosmetic units indicating more aggressive resurfacing for the lids and/or lips than surrounding cheeks and forehead.

Types of Combination Chemical Peel
• Superifical chemical peeling
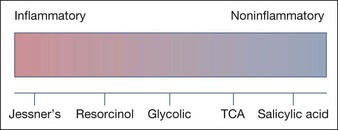
Each of these agents has its own characteristics and methodology and a physician must be thoroughly familiar with the chemicals, methods of application, and the nature of healing. The usual time for healing is from 1 to 4 days depending on the chemical and its strength. These agents range from noninflammatory (salicylic acid peels) to moderately inflammatory (Jessner’s solution) and each has a specific purpose (Fig. 14.3).
Sunscreens are necessary accompaniments to all peeling procedures and the patient should begin this prior to the peel. The proper FDA approved sunscreen should be chosen based on the patient’s skin type and procedure chosen. The choices are UVA filters, UVB filters and inorganic sunscreens (Table 14.4).
Table 14.4 Sunscreens and their photo protection
| Screens | UV protection (nm) |
|---|---|
| UVB | |
| p-Aminobenzoic acid (PABA) | 260–315 |
| Salicylates | 260–310 |
| Cinnamates | 280–310 |
| UVA | |
| Benzophenones | 270–350 |
| Meradimate | 336 |
| Avobenzone | 310–40 |
| Inorganic screens | |
| Titanium dioxide | 290–360 |
| Zinc oxide | 290–400 |
The peeling agent of choice to use for light pigmentary problems
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


