Fig. 4.1
Inspection of the breast. Left: static study of the profile and the surface of the skin (arms raised and lowered). Right: dynamic study, since contraction of the pectoralis muscles may accentuate clinical signs

Fig. 4.2
Minimal skin BC retraction (dimpling) noticeable when raising the ipsilateral arm

Fig. 4.3
Large retraction of the skin noticeable only when raising the ipsilateral arm
Finally, the patient should put her hands on her hips and press in to contract the pectoral muscles so that any other areas of retraction can be visualized. Inspection of the breast includes detection of asymmetry, bulging areas, skin changes (dimpling or retraction, oedema, presence of dermatological lesions), and position of the nipple (inversion or retraction, as in Fig. 4.4). Inspection should include peripheral areas (Fig. 4.5).


Fig. 4.4
Nipple partially retracted as a symptom of an underlying BC
Fig. 4.5
Very peripheral nodule (enlarging mass or extra-mammary thoraco-lateral lymph node?) of the left breast
PALPATION—A bimanual examination of the breasts should be performed while the patient is still in the sitting position, supporting the breast gently with one hand and examining the breast with the other hand (Fig. 4.6). The examination is completed with the patient’s arms raised above her head. This allows the examiner to flatten the breast tissue against the patient’s chest (Fig. 4.7).

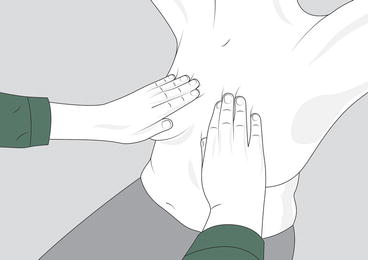
Fig. 4.6
Bimanual palpation in the sitting position to examine the deep and posterior layers of the breast tissue
Fig. 4.7
Bimanual palpation in the sitting position to flatten the breast against the chest wall and check glandular symmetry
In general, to examine the breast, use the pads rather than the less sensitive tips of the three middle fingers, with the hand slightly bowed (Fig. 4.8). Move the pads together as a single unit in a circular or radial way.

Fig. 4.8
Palpation with the finger’s pads starting from the clavicle towards the infra-mammary ridge. The pads of the second, third, and fourth fingers are the most sensitive. The pads of the fingers are rotated in concentric small (dime-size) circles for effective palpation of the breast. Do not pinch the breast tissue to avoid a false perception. Do not forget peripheral extension (axillary tail, subclavicular and parasternal regions)
Though many patients and some clinicians think of the breast only as the circular mound, breast tissue actually extends from the midaxillary line to the lateral edge of the sternum and from the clavicle to infra-mammary ridge. Covering the entire perimeter is essential in order to avoid missing peripheral areas, where a disease may occur, sometimes undetectable even on mammogram.
Use a consistent pattern that will cover all of the breast tissue within the borders of the perimeter. Begin the vertical strip pattern in the upper outer quadrant. Keep the pads perpendicular to the midaxillary line throughout the exam. Palpate up and down in overlapping strips, being sure to palpate each strip passed the infra-mammary ridge and up to the clavicle. To avoid missing an area, don’t lift your fingers from the skin. Be sure to include the nipple and sub-areolar area. Squeezing the nipple to illicit discharge is no longer a part of the screening CBE because only unilateral spontaneous discharge has any diagnostic significance for breast cancer. However, discharge should be investigated if reported by the patient.
The circular pattern follows the contour of the mound and tends to miss the peripheral areas, and also radial and wedge patterns show some limitations. What is important is that all the surface of the breast is examined, without missing any peripheral areas. With each palpation, push down through the entire depth of the tissue in three sequential manners:
Light: barely moving the surface of the skin
Medium: to the midlevel of the tissue
Deep: to the chest wall or ribs
Come back up through the tissue and slide to the next palpation. Using three levels of pressure will help detect asymmetric thickenings or masses that can occur at different depths in the breast tissue (Fig. 4.9). Keeping the hand bowed assures the use of pads which minimizes discomfort with depression. Repeating a mantra in your head of light, medium, and deep will help you to establish a rhythm. Be sure to elicit feedback from your patient regarding comfort level.
Fig. 4.9
Varying degrees of pressure are used (light, medium, deep) so that a small mobile mass is not pushed away by the palpating fingers
Palpation should include the careful application of pressure to the retroareolar region, including the lactiferous sinuses in that area, to check for abnormal discharge (Fig. 4.10). The patient herself is better able to apply concentric pressure to the retroareolar region than is a doctor seated in front of her. Thus, if questionable discharge is noted, the patient should compress the breast herself. If she has noticed the discharge at home, she has usually trained herself over a period of weeks to know exactly where she must push to elicit the discharge.
Fig. 4.10
Palpation of the retroareolar region. The structure of the nipple and areola complex (NAC) is different from the dominant breast tissue. The major duct area beneath the nipple is less dense and the hand detects as a hollow which is not easy to explore. Small masses may be missed or not easily detectable, unless using a technique that permits to flatten the area to the chest wall
Finally, a dimple indentation underneath the breast, if present, may be elicited by a lateral pressure, as shown in Fig. 4.11.

Fig. 4.11
Search for a dimple indentation underneath the breast elicited by a lateral pressure
The Cahan position




Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
