2 Choosing the Correct Peel for the Appropriate Patient
Introduction
Chemical peels are a method of resurfacing the skin. By inducing a controlled wound to the skin, chemical peels replace part or all of the epidermis and can induce collagen remodeling which helps to improve photodamage, rhytides, pigmentation abnormalities, and scarring. Chemical peels are divided into three categories depending upon the depth of the wound created by the peel (Boxes 2.1 and 2.2). Superficial chemical peels penetrate the epidermis only, while medium-depth peels damage the entire epidermis plus the papillary dermis to the level of the upper reticular dermis. Deep chemical peels create a wound to the level of the mid-reticular dermis. Each category of peel addresses a different aspect of photodamage and pigmentary abnormality. Healing time and complications vary among the different categories of peel as well, with some peels being more appropriate for certain skin types. Therefore, in order to maximize the benefits of a peel for a patient and to minimize adverse effects, it is important to choose which, if any, peel is appropriate for each patient. See also Box 2.3.
Evaluation of the Patient
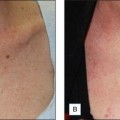
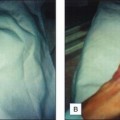
The physician should also perform a physical examination and pay particular attention to the patient’s skin type and degree of photodamage. Skin type can be classified using both the Glogau photoaging classification and the Fitzpatrick skin type scale (Box 2.4 and Table 2.1). Together, these skin classification systems can be used to objectively assess the patient’s skin and are an important component in choosing the appropriate peel. The Glogau photoaging classification system is used to quantify photodamage. Patients with Glogau type I skin would benefit most from a superficial peel, while those with Glogau type IV skin would benefit from deep peels. The Fitzpatrick skin type scale can be used to predict how a patient’s pigmentation will respond to each specific chemical peel. Patients with Fitzpatrick skin types I and II can usually be treated with all chemical peels safely and successfully, while care must be taken in those patients with Fitzpatrick skin types III to VI, since patients with these skin types have a much higher risk of developing postinflammatory hyperpigmentation (PIH; Fig. 2.1).