4
Chemical Peels: Superficial and Medium Depth
Chemical peeling began in ancient Egypt over 5000 years ago. Only fruit acids and lactic acids were then available. By the end of the nineteenth century, physicians started using other peeling agents, such as salicylic acid, resorcinol, phenol, and trichloroacetic acid. Phenol was first used to remove acne scars. The advent of alpha hydroxy acids (AHAs) and trichloroacetic acid has made chemical peeling a safer and more popular procedure.1
Laser technology has evolved rapidly, giving cosmetic physicians and their staff a new spectrum of treatments for skin rejuvenation. But chemical peels, still an effective therapeutic option for reversing photoaging, should not be forgotten. Their simplicity—ease of performance and low cost—make them an essential element in every skin care regimen. Physicians working with their aestheticians can offer their patients a variety of alternatives to achieve the best results, while recognizing the possibilities and limitations.
Superficial peels are recommended to treat a variety of superficial conditions involving the epidermis and superficial dermis: mild actinic damage, superficial wrinkling and dyschromia, actinic keratoses, and active acne. Series of peels are recommended, over specified periods of time. They require minimal or no recovery time and are rarely associated with adverse reactions or complications. And they can be used on patients of any skin type, particularly if notable inflammatory responses are avoided. Patients with tendencies for facial telangiectasias may find that these superficial peels and micro-dermabrasion may exacerbate their broken capillaries and are best avoided.2
Although effective in any age group, patients in their midthirties with early dyspigmentation, fine wrinkles, and mild actinic keratoses will find these peels a satisfying introduction to noninvasive facial therapies. With these peels we can achieve an improved appearance of the skin with more uniform color and texture and less visible pores. The effects are cumulative with time—augmented with the use of homecare products—and require maintenance. Superficial peels work well in combination with the other selections on the noninvasive facial rejuvenation menu—injectable therapies, intense pulsed light (IPL), and nonablative lasers. With the exception of acne rosacea patients, most patients can benefit from this procedure.
We use medium-depth peels primarily to treat moderate to severe dyschromia and moderate rhytidosis. It is an excellent therapeutic option for treating moderately photoaged skin, where the epidermis is atrophic and the stratum corneum thickened, and there are histologic findings of epidermal dysplasia, collagen, and elastin degeneration, translated as moderate facial rhytids. Severe photoaging is more predictably managed with carbon dioxide (CO2) laser resurfacing.
 Patient Selection
Patient Selection
The following criteria must be considered when making the patient/peeling agent selection:
- Fitzpatrick classification
- Age of the patient (younger patients respond better)
- Lifestyle (sun exposure, alcohol, drugs, smoking)
- Current skin care regimen
- Previous skin treatments (including other chemical peels, use of various lasers or other technology aimed at rejuvenation)
- Previous facial cosmetic surgeries
- Current medication
- Vitamin supplementation
- Previous history of herpes simplex (pre-treat with acyclovir or other antiviral agents)
- Realistic expectations and healing time
- Current skin care regimen
Once these variables are fully understood by the physician and patient, the physician will make the best recommendation, according to the specific needs and desires of the patient. The patients who require minimum recovery after the peel will receive superficial peels at regular intervals. The results will arise gradually, be limited to the surface of the skin, and, when combined with a good home care regimen, will provide a noticeable improvement (Figs. 4-1A,B; 4-2A,B). Patients that have severe epidermal damage extended to the superficial layer of the dermis and with coarse facial wrinkling are good candidates for medium-depth peels (Fig. 4-3A,B). The results will be dramatic, but with significant postpeel downtime, requiring at least 4 to 5 days of recovery. Postpeel home care speeds up recovery and emphasizes the importance of maintenance to maximize the results.
In summary, understanding the final histologic response to superficial and medium depth peels, the histological changes that occur during healing, and how much discomfort and downtime the patient is willing to endure, will allow the physician to appropriately select a peeling agent. The use of a prepeel regimen (lotions with low concentration of AHAs, retinoids, bleaching agents, topical antioxidants, and sunscreen) is highly recommended for at least 2 weeks prior to the peel. It prepares the skin for the treatment and also allows the physician to gauge if that patient can follow instructions and what kind of commitment can be expected from the patient to prolong and maximize the effects of the peel.3
 Superficial Peels
Superficial Peels
AHAs are the agents most frequently used in superficial peels. Often called fruit acids, AHAs are a group of naturally occurring substances found in food and in particular in fruits (glycolic acid in sugarcane, malic acid in apples, citric acid in citrus fruit). They are recommended for a variety of skin conditions but particularly those characterized by hyperkeratinization (the fine wrinkling associated with photodamage and acne).
Glycolic acid is the most used AHA, and even though its mechanism of action is not totally understood, it has an effect in disrupting keratocyte cohesion and therefore correcting an abnormally thickened stratum corneum. By creating a thinning of the stratum corneum, AHA improves the general texture and uniformity of the skin, facilitating the penetration of other topical agents (such as Retin-A). Also, by increasing the hydration of the stratum corneum and stimulating synthesis of cellular ground substances (glycosoaminoglycans), AHAs reduce fine wrinkling.

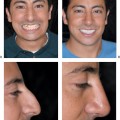
Figure 4-1 (A) This patient exhibited superficial facial contour irregularities and irregular pigmentation. (B) After multiple series of alpha hydroxy acid (AHA) peels of increasing strength and daily use of home care products (containing AHA, retinoids, hydroquinone, vitamin C) there is a marked improvement in this patient’s skin texture and pigmentation.

Figure 4-2Alpha hydroxy acid peels and homecare products can yield significant benefits in patients of all skin types. (A) This patient with skin type IV had superficial contour irregularities and irregular pigmentation. (B) She noted a significant improvement in her skin texture and pigmentation after treatment.
As a peeling agent, AHAs can be found as a solution or as a gel, and are used in concentrations of 15 to 30% (by aestheticians) and 50 to 70% (by physicians). They are systemically safe, nontoxic acids, produce few complications, and offer instant gratification. They have to be neutralized to terminate their action, either by rinsing them off with water or by applying other neutralizing solutions.
Factors affecting the depth of penetration of a glycolic peel are the concentration, method of application, skin pretreatment, and duration of the acid in contact with the skin.
Other superficial peeling agents include trichloroacetic acid (TCA) in concentrations 10 to 20%; salicylic acid 50%; and Jessner’s solution [resorcinol 14 g, salicylic acid 14 g, lactic acid 14 g, ethanol (95%) in 100 mL].

Figure 4-3 (A) Although contemplating a rhytidectomy for facial skin redundancy, laxity and rhytidosis, she pursued a noninvasive approach. (B
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


