Fig. 1
(a, b) Salicylic acid peel at 30 % in ethanol for inflammatory acne. The image (b) shows the whitish precipitation of the acid
There is, then, moderate burning which gives in a few minutes, leaving a feeling of light anesthesia in treated area. Small frostings (level 1) can be seen in the areas of inflammatory acne lesions, not requiring neutralization. The excess of white precipitate is removed, after 5–10 min with water or cleansing lotion. In 3–5 days, very fine whitish scaling occurs.
Symptoms of salicylism, while rare, may occur, ranging from light (rapid breathing, tinnitus, hearing loss, dizziness, nausea, vomiting, and abdominal pain) to severe (central nervous system changes simulating alcohol intoxication). For this possibility, the use of this substance is only recommended on smaller surfaces such as neck and presternal region (Brubacher and Hoffmann 1996). Recently, a new preparation containing 30% salicylic acid in a polyethylene glycol (PEG)-based vehicle has been used with good clinical results in volunteers with aged skin, showing improvement in skin texture, and in acne patients with disappearance inflammatory acne and comedones. For being little volatile, PEG has a higher affinity for salicylic acid and thereby releases it only in small amounts in the superficial layers of the epidermis. This affinity justifies lower absorption of the substance, with lower systemic toxicity as well as a reduction of burning sensation during application (Dainichi et al. 2008). On the other hand, salicylic acid formulated in ethanol, being highly lipophilic, has high affinity for the pilosebaceous units, providing certain dryness desirable in patients suffering from body acne (Peterson and Goldman 2011).
Jessner Solution
Jessner solution consists of 14% salicylic acid, 14% lactic acid, and 14% resorcin in ethanol. The solution has keratolytic, anti-inflammatory, and lightening action. Depending on the number of layers applied on the skin surface and volume used, it acts as a peel that extends from very shallow to medium depth. The penetration is determined partially by the epidermolytic action of lactic acid that, despite being low in concentration, depends on the pH for its release in the formulation.
This peel serves as an adjunct in the treatment of inflammatory acne in areas of hyperchromias on the trunk (anterior and posterior), especially in higher skin types. In such cases, it is preferable to apply it with gauze, exerting some pressure, especially on areas with thicker corneal layers and more numerous sebaceous structures. This peel is also indicated for the treatment of rejuvenation of the neck and colo, but with fewer layers. It avoids therefore an unnecessary depth of the peel (Peterson and Goldman 2011; Brody 1997; Fig. 2a–c).
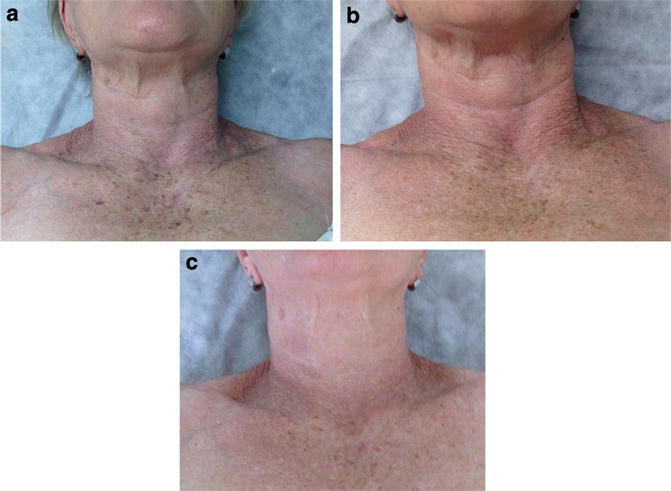
Fig. 2
(a–c) Jessner peel (three layers) for moderate photoaging. (a) Before the procedure, (b) after the first session (14th day), and (c) after two sessions (40th day)
The Jessner peel is usually very well tolerated by patients, causing mild to moderate stinging, which lasts between 3 and 10 min. After application, there is slight whitening of the skin, due to the precipitation of salicylic acid, followed by variable erythema with light frosting areas (levels 0 to 1). It is recommended to wait 3–4 min between applications of layers, so there is evaluation of the extent of the peel already performed. This is a peel that does not require neutralization. The precipitated salicylic acid can be removed with water or cleansing lotion. Between 3 and 5 days, clear to brown flaking occurs. The Jessner solution should be used in fortnightly or monthly intervals, for three to six sessions.
The Jessner peel is considered to be very safe: the allergic reaction, determined by hypersensitivity to resorcin, has low incidence, and the treatment has little toxicity, due to the low concentration of resorcin and salicylic acid in the formulation. For added security, it is recommended to perform rotation of treated areas, between procedures. This guidance also applies to all other peels that have some degree of systemic absorption of used agents (Table 1).
Table 1
Rotational treatment in body peels
Rotational treatment – body peel | |||
|---|---|---|---|
Period | Area of treatment | Peel type | Interval/number of sessions |
First week | Chest and neck | Jessner solution, glycolic acid | Monthly or bimonthly/3–6 |
Second week | Back of hands and forearms | Trichloroacetic acid, Jessner solution | |
Third week | Shoulders and arms | Salicylic acid | |
Fourth week | Thighs and legs | Thioglycolic acid | |
Resorcin
Resorcin is a caustic agent from the group of phenols, soluble in water and alcohol, used in scrub solution or paste, at concentrations ranging from 10% to 50%. In very superficial body peels , especially for acne on anterior and posterior trunk, the use at lower concentrations is more appropriate, between 20% and 30% (5–10 min) (Clark and Scerri 2008). It can be used in combination with the sulfur, both at 24% solution in distilled water (Kede 2009). This peel is also indicated for the treatment of dyschromia, fine wrinkles, and post-inflammatory hyperpigmentation. Consider taking the pretest as it can cause contact dermatitis (Kede 2009). Special care must be taken in higher concentrations and when applied in more extensive body areas.
Tretinoin
Tretinoin, also known as retinoic acid, is a drug of the class of retinoids used for superficial peels. This peel is formulated in a yellow solution in propylene glycol; the used concentrations range from 5% to 12%. To obtain a cosmetic effect, tint may be incorporated to the formula. This peel is widely used in cosmetic dermatology by a combination of factors: the ability to promote thinning and compaction of the stratum corneum, reverse atypia in epidermal cells, stimulate neocollagenesis in the dermis, increase the deposition of glycosaminoglycans, stimulate the reorganization of collagen fibers damaged by sun exposure, and remove and disperse the melanin granules formed in keratinocytes (Kede 2009). Its use is widespread in photoaging treatments and actinic skin changes (e.g., poikiloderma of Civatte) (Landau 2008), in pigmentation disorders such as post-shaving folliculitis, acne, insect bites, and melasma in non-facial areas, and in traumatic injuries, especially in trunk regions and upper and lower members. In the treatment of acne, it corroborates with home-based use of tretinoin promoting the elimination as well as the prevention of follicular hyperkeratosis.
The tretinoin peel is often used after microdermabrasion with aluminum oxide crystals in which the stratum corneum is removed mechanically. This combined procedure optimizes the therapeutic results with an epidermal deepening (Hexsel et al. 2005). The indication extends to the treatment of the old stretch marks, of pearly color, as well as those of recent emergence, in pinkish color. For this purpose the concentration should be of 10%, for a contact period of 4–6 h until the removal with water (Kede 2009). This peel is recommended after procedures like electrocoagulation or cryosurgery of epidermal growths such as seborrheic and actinic keratosis, milia, sebaceous hyperplasia, and papulosis nigricans. Studies show that this association seems to provide a better healing (Hung et al. 1989), promoting uniformity of skin tone and improvement in skin quality.
The tretinoin peel is painless and easy to perform. The chemical agent is applied with the help of a gloved finger. In the mean interval of 3–4 days, there is a white desquamation, dry, fine, and proportional to the concentration and length of exposure to the substance. The application, in a biweekly or monthly interval, is completely painless, because tretinoin has no acidic pH capable of promoting protein coagulation. Being a photosensitive drug, it should be applied late in the day and remain on the surface for at least 6 h (Landau 2008). For best results it is possible to perform a gradual increase of the length exposure in each application from 4 to 12 h limit. This peel is not recommended for pregnant women and should not be carried out throughout the breastfeeding period (Fig. 3a–c).
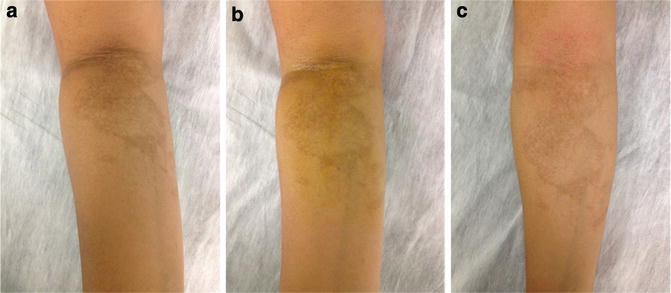
Fig. 3
(a–c) Tretinoin peel at 5% in propylene glycol for traumatic post-inflammatory hyperpigmentation. (a) Before the procedure, (b) immediately after the procedure, and (c) after the first session (14th day)
5-Fluorouracil
5-Fluorouracil (5-FU) is a fluorinated pyrimidine from the group of antimetabolites which acts as a cytostatic agent in the treatment of preneoplastic and neoplastic cutaneous diseases. It is also called fluorouracil-pulsed peel and consists of a combing two superficial peel agent. Usually it is combined with Jessner or glycolic peel. The first step begins with the Jessner solution or with glycolic acid 70% in fluid gel. When starting with the Jessner solution, it is recommended to apply one or two layers to reach an initial (level 0) erythema or salicylic precipitation, not requiring neutralization. In the case of the glycolic acid, neutralization with water or sodium bicarbonate is required. Then, 5% 5-FU is applied in propylene glycol or cream on a body surface which should not exceed 500 cm2 (about 23×23 cm) leaving it to act for 6–12 h.
This procedure is performed in weekly or biweekly interval, until eight pulses, for the treatment of multiple actinic keratoses. In a study conducted by Katz (1995), the combined peel with the Jessner solution has enabled a reduction of 86% of studied injuries; in another study, Marrero (1998) obtained the best results, with 92% injury reduction with the combination with glycolic acid at 70%.
Glycolic Acid
Glycolic acid (GA) has its natural source in sugarcane, being produced in the laboratory for use as a chemical peel. It has one of the smallest molecule sizes among the alpha hydroxy acids. Therefore, the penetration of GA in the skin occurs, compared to other alpha hydroxy acids, more easily. GA can be used as very superficial or superficial peeling agent, depending on the concentration used, the pH of the formulation, and the exposure time on the surface (Clark and Scerri 2008; Fischer et al. 2010). The concentration of 70% in pHs lower than 1.0 can become a medium-depth peel, depending on the exposure time on the skin. The higher the concentration of GA, at a lower pH and at longer exposure, the deeper is the peel. This is due to the greater bioavailability of the chemical in these conditions (Kede 2009).
This peel is indicated as an adjunct in the treatment of non-facial areas for photoaging, inflammatory acne, and atrophic acne scars and in pigmentary disorders such as melasma and post-inflammatory hyperpigmentation (Clark and Scerri 2008; Takenaka et al. 2012; Callender et al. 2011). Good clinical results can also be achieved in the treatment of folliculitis and pseudofolliculitis of groin and buttocks. The GA’s action results from compaction effect of the stratum corneum, epidermal thickening, and dermal deposition of collagen and mucin.
The GA peels are sold as free acids, partially neutralized. There are different manufacturers with different pHs ranging from 1.0 to 3.0. Some formulations have even lower pH around 0.6. The lower the pH, the greater the amount of acid in the free form, allowing to deeper penetration into the skin with formation of faster and more extensive frostings. These frostings show areas of cell epidermolysis, color ranging from white to grayish white, according to the dermal penetration of GA (Clark and Scerri 2008). In areas with increased thickness of the stratum corneum, formulations with lower pH (0.6–1.0) can be chosen, in order to facilitate penetration of the acid without compromising the security of the application. All peels with alpha hydroxy acids require neutralization when the desired depth is reached. This is done using an alkaline solution or water. It’s preferable to use sodium bicarbonate at 10% in fluid gel as neutralizing agent because, by having a clearly alkaline pH, it promotes certain effervescence in the place to be neutralized when in contact with the acid pH of the peel. This effervescence provides better control over the peel, reaching the exact depth we desire.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


