18 Cheeks
Summary and Key Features
• The cheeks are important to communicating one’s age and are essential for smiling and laughing. Filling the cheeks reconstitutes a youthful appearance, and adds value to rejuvenation of other facial cosmetic units
• Anatomical borders are: the zygomatic arch, inferior orbital rim, lateral nose, nasolabial fold, and superior jawline
• Aging causes facial bone and soft tissue atrophy. It accentuates gravitational descent of the angle of the mouth and produces unattractive shadows. Lipoatrophy is associated with an unhealthy appearance
• Fat augmentation of the cheeks is a well-established technique. It offers excellent cosmetic results, but requires donor tissue and may not be long lasting
• Non-resorbable fillers provide long-term results, but have permanent risks
• Resorbable fillers are excellent options for cheek augmentation. They allow office-based procedures yielding natural results, and are increasingly long-lasting with minimal risks
Introduction
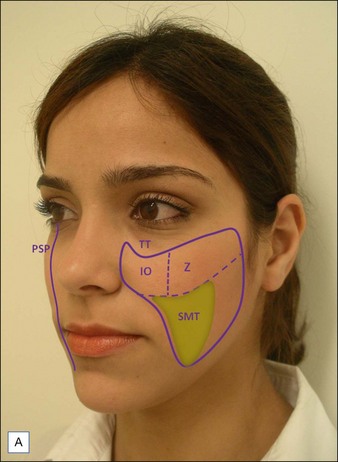
Each cheek is composed by the soft tissues covering the paramedian central facial skeleton (Table 18.1). The upper third of the cheek can be further divided into zygomatic and infraorbital subunits. The zygomatic subunit (cheekbone) represents the area of maximal projection of the cheek, called the malar eminence (Fig. 18.1A). The ideal malar eminence diffusely reflects light regardless of the angle one looks at the face. The cheeks work as a frame for adjacent cosmetic units such as the lips, eyes, and ears, allowing the observer to instinctively calculate cosmetic ratios related to those structures.
Table 18.1 Borders of the cheek
| Adjacent anatomical units | |
|---|---|
| Superior | Zygomatic arch; inferior orbital rim |
| Medial | Lateral nose; nasal–labial folds |
| Lateral | Preauricular sulcus |
| Inferior | Above the inferior jawline |
| Internal | Oral cavity, maxillary, and zygomatic bones |
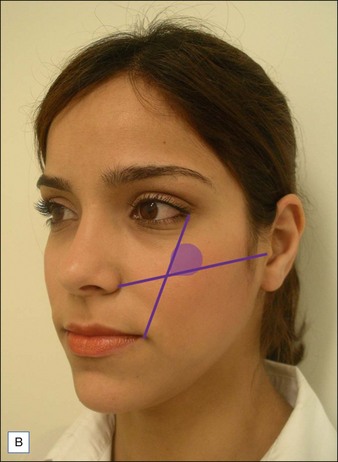
Although prominent cheekbones are usually associated with beautiful individuals, it is their relationship with the other facial structures that defines attractiveness. Several techniques are available to identify the optimal location of the malar eminence. Hinderer’s method is easy to obtain, helping to optimize filler placement when augmenting the cheeks. The ideal reflection of light should be kept in the upper outer quadrant formed by the intersection of two virtual lines: the first one runs from the lateral canthus of the eye to the angle of the mouth; the second one goes from the nasal crease to the tragus. Other aesthetic features of the cheeks are superficial textural homogeneity, lack of shadows, and smooth transition towards adjacent cosmetic units. Accordingly, the ideal parasagittal profile contour should have a smooth curvilinear shape from the eyelids to the cervical jaw angle (Fig. 18.1B).
Aging of the mid-face is essentially caused by atrophy of the cheek bones and fat pads. In two areas these changes are striking: (1) within the submalar triangle (an inverted triangle defined medially by the nasolabial fold, superiorly by the malar eminence, and laterally by the anterior border of the masseter muscle) and (2) along the tear trough and eyelid / cheek junction. These changes lead to a deflated balloon pattern – folding the overlying skin. In addition, mid-face atrophy loosens the tissue surrounding the angle of the mouth, leading to a sad appearance (Fig. 18.2A). Filling the cheeks helps in restoring a gracious oral commissure (Fig. 18.2B).

Autologous fat transfer offers excellent overall cheek augmentation (Fig. 18.3). However, it requires harvesting of tissue, which may be difficult to obtain in the presence of generalized fat loss, as seen in some patients with drug-related HIV lipoatrophy. The duration of fat grafts is variable according to the technique used and recipient area (the cheeks usually have good retention rates); it also varies among individuals. Coleman reported that injecting small droplets of donor tissue, so that the whole graft receives enough nutrients, improves graft survival. Sterodimas et al found that adipose-derived stem cell-enriched lipografts may also prolong results. Despite those advances, liposculpture may not be attractive to individuals looking for office-based procedures.


 This chapter and attached video focus on using HA for mid-face augmentation. PLLA and hydroxylapatite are briefly discussed.
This chapter and attached video focus on using HA for mid-face augmentation. PLLA and hydroxylapatite are briefly discussed.Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


