In my practice, cheek implants (Fig. 14.1) are rarely indicated. Particularly as the procedure applies to the malar mound, I find it rarely necessary in facelift surgery. Rather, I have found that repositioning/uplifting tissues (that once covered the malar prominence and have descended because of aging) by performing a cheek lift creates the aesthetic enhancement that most patients require (see Chapter 20 on facelift surgery).
At the time of this writing, I am not a strong advocate of temporary fillers or fat grafting for this region, if the patient is amenable to surgery. I prefer to “volumize” the region by replacing the fat/soft tissue mound to its original position with a cheek lift procedure. I have found this practice not only to be more effective, but also to be the most predictable and economical method of re-creating a youthful “midface” (Fig. 14.2).
When a malar implant is advised, I generally prefer the “anatomical” silastic model, inserted through an intraoral incision made vertically at the gingival-mucosal sulcus, superior to the canine (cuspid) teeth. It is the incision preferred when open maxillary sinus antrostomy is performed. The implant is inserted using the same “no-touch” technique described with chin implants in a subperiosteal fashion, after a “made-to-size” pocket is created. The incision site is closed with an absorbable suture (usually chromic catgut.)
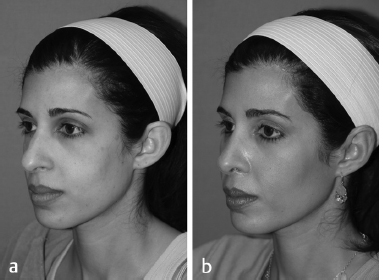
Fig. 14.1 (a) Before and (b) after photos of a patient who underwent cheek/malar augmentation with silastic implants.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


