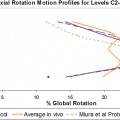
12 A surgical option besides fusion for cervical disk disease has been elusive until recently. With advances in biomechanics and design philosophy, disk replacement surgery has emerged to provide a viable alternative to fusion surgery. The force advancing this “motion preservation” philosophy is the theoretical prevention of adjacent segment disease that is purported to occur after fusion of a motion segment. Several theories have implied that fusion is directly related to the development of adjacent disease. Cadaver studies have shown that disk pressure above and below a simulated fusion segment during flexion increase 73% and 45%, respectively.1 Motion at a segment adjacent to a fusion also increases up to 40%.2 It is believed that the use of a total disk replacement system can preserve physiological motion at adjacent levels. This has been postulated to prevent disk disease at a normal adjacent level and reduce the morbidity and poorer outcomes of revision surgical procedures. Other benefits of disk replacement surgery include maintenance of a physiological range of motion, decreased morbidity related to fusion procedures, and an earlier return to function and activity. The CerviCore Cervical Intervertebral Disk Replacement prosthesis (Stryker Spine, Allendale, NJ) was developed with an innovative saddle-shaped articulation (Fig. 12–1). It is a cobalt chromium metal-on-metal articulation that more closely matches physiological motion than constrained ball and socket or single center of rotation designs. From C3–C4 to C6–C7 in the cervical spine, maximum range of motion in flexion-extension is 10 degrees. In lateral bending and axial rotation, it is 11 degrees and 7 degrees, respectively.3 The center of rotation is in the superior vertebral body during lateral bending and in the inferior body during flexion-extension (Figs. 12–2 and 12–3). The motion provided by the opposing saddle-shaped bearing surfaces is 7.5 degrees in both flexion-extension and lateral bending (Fig. 12–4
CerviCore Cervical Intervertebral
Disk Replacement
Design Philosophy
Related posts:
 Prosthetic Disk Nucleus Partial Disk Replacement: Pathobiological and Biomechanical Rationale for Design and Function
Prosthetic Disk Nucleus Partial Disk Replacement: Pathobiological and Biomechanical Rationale for Design and Function
 Bryan Cervical Disc Device
Bryan Cervical Disc Device
 Spinal Kinetics Cervical Disc
Spinal Kinetics Cervical Disc
 Biomechanical Testing Protocol for Evaluating Disk Arthroplasty
Biomechanical Testing Protocol for Evaluating Disk Arthroplasty
 DIAM (Device for Intervertebral Assisted Motion) Spinal Stabilization System
DIAM (Device for Intervertebral Assisted Motion) Spinal Stabilization System
![]() Nonfusion Stabilization of the Degenerated Lumbar Spine with Cosmic
Nonfusion Stabilization of the Degenerated Lumbar Spine with Cosmic
![]()
Stay updated, free articles. Join our Telegram channel
 Design Philosophy
Design Philosophy Materials Testing
Materials Testing Preclinical Testing
Preclinical Testing Current Clinical Trials
Current Clinical Trials Conclusion
Conclusion
Full access? Get Clinical Tree


