Major indications
Advantages
Disadvantages
Lesions characterised by a liquid component and/or necrosis features (complicated cysts, some papillary lesions)
Anyway established diagnosis (benign or malignant)
Localisation of the lesion in some challenging areas as axilla, close proximity to the chest wall or breast implants
Cheap
High sensitivity
Provides diagnosis in most common instances
Can be referred immediately
Operator dependent
Needs experienced cytopathologist
Painful
Cannot differentiate invasive from in situ cancer
Variable percentage of C1 (inadequate or insufficient)
Few, but possible, false positives
Core needle biopsy (CNB) provides increased sensitivity and specificity compared to fine needle aspiration cytology. Sensitivity and specificity are related to the size of the needle. CNB using a 14- or 16-gauge needle is widely accepted to be sensitive (90 %) and specific (98 %) in diagnosing breast masses, compared with 60 and 86 %, respectively, for FNA. In any case, CNB is recommended in most doubtful cases and mandatory for lesions as architectural distortion and microcalcifications.
Diagnosing lesions with needle biopsy has several advantages. For benign lesions, establishing a definitive diagnosis obviates unnecessary surgical excision or protracted follow-up, both of which are costly in psychosocial and resource terms. A definitive diagnosis of cancer allows the patient to make an informed choice and to obtain counselling before surgery (Table 6.2).
Table 6.2
Indications, advantages and disadvantages of core needle biopsy (CNB)
Major indications | Advantages | Disadvantages |
|---|---|---|
Findings highly suggestive or suspicious for malignancy (BIRADS 4/5) or assessed as probably benign (BIRADS 3, C1 and C3 cytological class) Multicentric lesions in order to plan timing and way of treatment Results not correlated with the clinical and imaging findings | Easy to perform High sensitivity, more high specificity with close to zero false-positive rate Provides a definitive histological diagnosis Facilitates in the planning of multimodal treatments for women with BC or who refuse surgery or when surgery can be avoided (very old women) | Operator dependent Cannot easily be reported immediately Uncomfortable but less painful than FNA Bruising and swelling |
Vacuum-assisted biopsy (VAB) is a more complex and expensive percutaneous needle biopsy technique. It should be reserved for large sampling as needed in some clusters of microcalcifications or in some radiological areas with architectural distortion. The procedure is accurate as when a tissue sample is removed surgically.
The core needles are of a large calibre and are mounted onto a spring-loaded device that allows small cylinders of tissue to be cut and collected within the notch of the needle. Technically, the best core biopsy samples are obtained by using 8- or 11-gauge needles. The optimal number of passes required varies according to the mammographic appearances of the lesions being sampled, with fewer passes required for solid lesions compared with microcalcifications. Several investigators have shown that a minimum of 5–6 passes is required when sampling microcalcifications to minimise sampling error. In case it is performed for microcalcifications, a wide-bore needle should be preferred; moreover, a specimen radiography of the cores should be obtained to demonstrate the presence of calcifications.
VAB may be an alternative to open surgery for additional tissue biopsy in patients with microcalcifications or borderline breast lesions. Compared with open surgical biopsy, needle biopsy is cheaper, it causes less trauma and disfigurement, no breast defect remains, and unlike with surgery, it does not distort the breast tissue making it difficult to read in future mammograms (Table 6.3.)
Table 6.3
Indications, advantages and disadvantages of vacuum-assisted biopsy (VAB)
Major indications | Advantages | Disadvantages |
|---|---|---|
Clusters of indeterminate microcalcifications An architectural distortion in the structure of the breast tissue An area of diffuse non-specific abnormality Failed ‘conventional’ core biopsy Some papillary and mucocele-like lesions | An excellent way to evaluate microcalcifications Generally, the procedure is not painful and the results are as accurate as when a tissue sample is removed surgically | Because device removes larger pieces of tissue, there is a risk (less than 1 %) of bleeding and forming a hematoma, at the biopsy site An occasional significant patient’s discomfort can be readily controlled by pain medication |
Undoubtedly, VAB is advantageous in increasing the preoperative diagnostic accuracy of impalpable breast lesions and even in reducing the overall costs of diagnosis compared with surgical excision. Even so, each new and incremental development has increased the cost of the procedure; it is therefore prudent to use a biopsy technique with full knowledge and awareness of the individual strengths and weaknesses of not only the individual capability, but also the expertise available in one’s institution.
According to all-purpose available expertise, masses may be successfully sampled with FNA or core biopsy under ultrasound guidance, whereas stereotactic vacuum biopsy of small clusters of indeterminate microcalcifications may be more appropriate as a modality of choice compared with FNA or core biopsy. Used in this manner, image-guided percutaneous needle biopsy can be used effectively to ensure that most palpable and impalpable breast lesions are diagnosed with accuracy and certainty.
Open surgical biopsy. Some large lesions which are predominantly architectural distortion should be subject to excision biopsy, following preoperative diagnostic workup. That is due to a significant risk of associated malignancy which may not be demonstrated even under ideal sampling conditions. Also, lesions that are proven with atypical ductal hyperplasia (ADH) or radial scar (RS) should be subject to excision due to the risk of associated malignancy (Table 6.4).
Table 6.4
Indications, advantages and disadvantages of open surgical biopsy
Major indications | Advantages | Disadvantages |
|---|---|---|
Clinical suspicion of malignancy not otherwise confirmed by sampling, especially when a mastectomy or axillary clearance is planned Large benign lesions, i.e. benign phyllodes tumours or large fibroadenoma Diagnosis of atypical hyperplasia done on CNB Diagnosis of radial scar done on imaging and CNB Every papillary lesion ascertained Suspicion of malignancy on one or more investigations with indeterminate or inadequate CNB, usually in patient with screen-detected microcalcifications Request by the patient | Preoperative triple diagnostic assessment should be achieved in most cases, but few conditions require an unquestionable definitive surgical diagnosis | A surgical biopsy has more physical and psychological consequences than other procedures It is expensive and it will leave a scar The more tissue removed, the more likely a change in the shape of the breast could be noticed All biopsies can cause bleeding and swelling and carry a mild risk of infection |
Sampling techniques should be carried out with due regard to the imaging or to clinical finding, starting from the most suspicious features. Where there is a possibility of discordant clinical and imaging findings with regard to any lesion, it is worthwhile to carry out sampling under both imaging and clinical guidance.
Ultimately, each type of biopsy has its pros and cons (Fig. 6.1). The choice of which type to use depends on many factors: how suspicious the tumour looks, how big it is, where it is in the breast, how many tumours there are, personal preferences and other medical and ethical aspects related to the patient.
Fig. 6.1
Different types of needle biopsy of the breast. FNA (fine needle aspiration): operator-dependent technique with multiple needle insertions and small samples. Core needle biopsy (CNB): few insertions, larger sample size and accurate histological diagnosis. Vacuum-assisted needle biopsy (VAB): several large samples with one needle insertion
6.2 Cytological Samples
Clinical Practice Points
FNA is an operator-dependent technique. Moreover, the reporting of breast cytological results is more demanding than histological analysis.
Proper targeting of localisation by the operator and experience of the pathologist in handling and interpreting cytological samples make the difference in the results.
FNA cannot reliably distinguish preinvasive from invasive cancer, nor does it provide sufficient tissue for testing cancer by immunohistochemistry.
Besides FNA, cytological samples can be obtained by nipple discharge and by exfoliated cells of the surface of the nipple.
6.2.1 Fine Needle Aspiration (FNA)
In many cases, fine needle aspiration (FNA) remains an important tool in the assessment of breast diseases. FNA and core needle biopsy (CNB) are currently the standard for triple assessment diagnosis. The use of FNA does confer a couple of advantages: it is inexpensive and quick to perform. The results can be made available rapidly, enabling a one-stop diagnostic and results clinic. This approach has an accuracy of over 90 % for palpable breast lesions when all three components are concordant for benign or malignant disease. However, accuracy falls in as many as 40 % of cases where the findings are not concordant.
FNA is simple to perform, but truthful diagnosis depends on a number of factors, such as knowledge of the correct techniques and their application, use of the most appropriate technique for a particular clinical situation, sensitivity and specificity of the method and interpretation of results in the setting of clinical findings. FNA is definitely an operator-dependent technique. Moreover, the reporting of breast cytological results is more demanding than histologic analysis, and the degree of expertise required is not always available.
Findings from cellular samples are limited in that the reviewer may not be able to determine the grade or invasiveness of the tumour. It is also difficult to diagnose a lobular carcinoma on the basis of cytological results. Nevertheless, there is evidence to indicate that ultrasound and FNA biopsy are similarly useful for the axillary staging of patients with invasive carcinoma.
The technique of FNA is largely determined by the individual surgeon’s preference, which may, in part, reflect hand size and individual technique. A 21-gauge (green) needle is used most commonly, although in expert hands, a 23-gauge (blue) needle can yield as much information, with less discomfort and bruising. Some clinicians opt for a hand-held 10-ml syringe, whereas others prefer a 20-ml syringe used with a syringe holder. Syringe holders allow a vacuum to be easily maintained but can make control of the needle tip less precise.
To perform FNA, the needle is passed through the lesion a number of times while maintaining suction and steadying the breast tissue with the other hand. Considering the potential risk of pneumothorax, it is important when performing needle biopsies of the breast, and wherever possible, to angle the needle tangentially to the chest wall (Fig. 6.2).

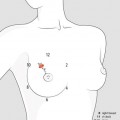
Fig. 6.2
Fine needle aspiration of peripheral breast mass. In order to avoid a risk of pneumothorax, it is advisable to insert the needle diagonally
When the mass is near to the chest wall, it is better to move it laterally to a position over the rib (Fig. 6.3) or to use a needle alone (Fig. 6.4).
Fig. 6.3
Fine needle aspiration of a breast mass. The mass is trapped between the pads of the index and the middle finger of the nondominant hand and the needle introduced vertically. In some cases, it is advisable to move the mass laterally to a position over the rib. For most lesions, it is cautious to use ultrasound guidance or outlining the lesion with a marker pen
Fig. 6.4
Fine needle aspiration of small superficial breast mass. A better control of the core insertion could be obtained using a needle alone. If the needle is slowly moved up and down with a little rotation, an appropriate sample could be obtained with no suction for negative pressure
Sampling should be continued until aspirate is observed at the bottom of the plastic portion of the needle. Finally, the aspirate is transferred to slides and spread in a way thin enough to visualise individual cells. According to the preference of the local laboratory, the slides may be air-dried or fixed by immersing the slide(s) in alcohol for 30 s or by using the cytology spray fixative. In some cases, the presence of the cytologist is advisable at the time of sampling in order to immediately verify its adequacy.
Free-hand insertion. If the area to be biopsied can be felt, the needle is manually directed towards the suspicious area. The sample should be obtained with the needle inside the lesion by rapid and multiple inward and outward movements associated with rotations, to ensure a representative collection of cells. Before removing the needle, it is very important to take good care of interrupting the suction.
Ultrasound (US) guidance is generally preferred when the lesion is best visible with ultrasounds. In small lumps, the depth of the mass is misleading, and only US can guide the needle towards the centre of the lesion. An outpatient breast clinic should always have an US equipment. It is low cost and rapid and provides high-precision guidance in all kinds of sampling.
Stereotactic directional guidance. In cases of non-palpable lesions visible only on mammograms, such as small opacities or small cluster of microcalcifications, stereotactic directional guidance should not be used, other than for a guided localisation (see Sect. 6.4).
6.2.2 Nipple Fluids
Nipple discharge. Nipple discharge occurs when fluid inside the ducts is elicited by expression of the nipple or when it spontaneously flows from the nipple. Nipple secretions can be expressed in up to 85 % of women and are generally the by-products of ductal epithelial cells undergoing cellular turnover.
Cytological investigation of nipple discharge is commonly done when spontaneous discharge comes from only one nipple orifice. The fluid is collected in one or more slides and immediately fixed by immersing the slide(s) in alcohol for 30 s or by using the cytology spray fixative. For cytology of nipple fluids, it is better to collect the final (not the first) fluid elicited by a gentle expression of the nipple and not to allow the material on the slide to dry prior to fixation.
Nipple aspirate fluid (NAF) and ductal lavage (DL) are considered new approaches to cancer prevention in high-risk patients with family history of BC. The majority of BCs originate in cells that line the inside of the milk ducts in the breast. The presence of atypical cells from nipple or fine needle aspiration has been linked to an increased risk of cancer within 3–5 years following testing, and it is generally assumed that atypical cells obtained using ductal lavage would indicate a similar risk. However, because fluid is not usually collected from all of the milk ducts during these procedures, it is unclear what conclusions can be drawn if no atypical cells are present in a sample.
Nipple aspirate fluid (NAF) is a minimally invasive procedure based on gentle suction to collect fluid from the nipple. This is done with a device similar to breast pumps used by nursing women. Fluid containing cells from the lining of the ducts can be obtained from about 75 % of women, but only a tiny amount of fluid and a few cells can be obtained.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


